|
"Only a small fraction of oocytes will reach the correct maturation stage and acquire the potential to be released and fertilized". Author: Edel Rocher 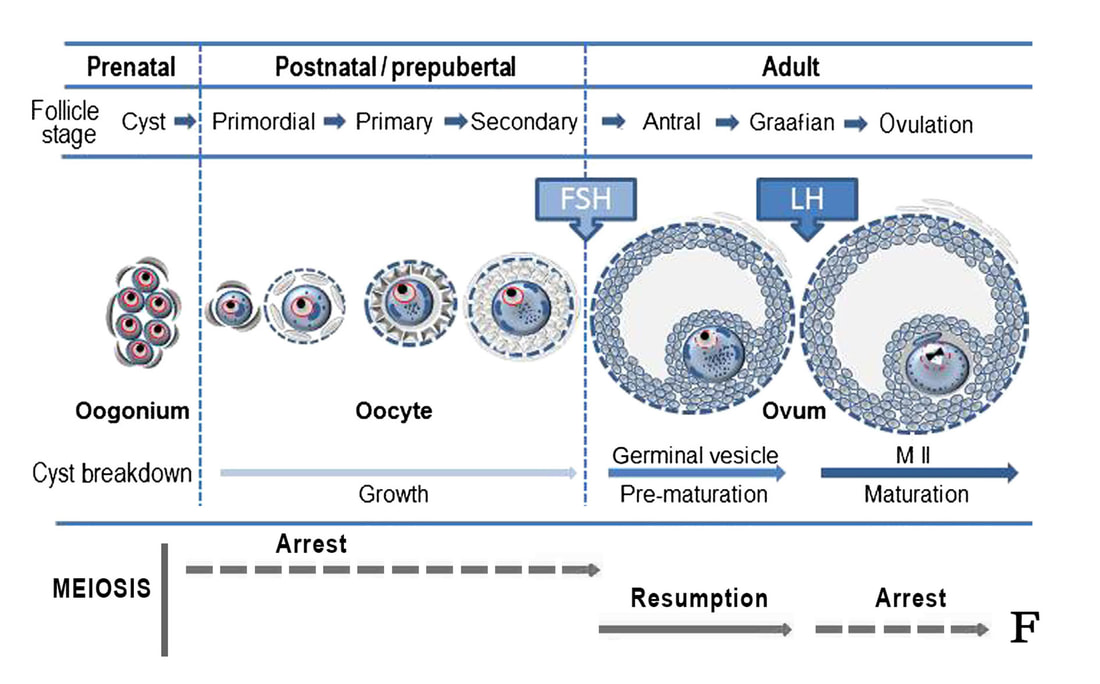 Figure 1. Representation of the parallel growth of follicles and maturation status of oocytes. During embryo development, germ cells are associated to each other in multinucleated cell accumulation called cysts. Each of these cysts contains multiple oogonia, the cells that will eventually become the oocytes. At birth, oogonia are already individualized as oocytes and surrounded by ovarian cells, forming a structure called primordial follicle. Some of the follicles eventually grow due to proliferation of the oocyte-surrounding cells (follicular cells), while oocyte development continues. For this to occur, an intricate balance of hormonal actions is needed, whose main characters are FSH and LH (modified from [1]). During assisted reproduction treatments ("cycles"), immature oocytes (or eggs) are oftentimes found. The following lines try to explain the reader why these cells are so frequent, and why they reduce the success rates of fertility treatments. The egg or oocyte is part of a cell aggregation found in the ovary referred to as follicle. Follicles receive and produce a series of hormone secretions that contribute to the maturation of these eggs, which are eventually released during ovulation. At birth, women normally present somewhat between 1 and 2 million ovarian follicles. These are called primordial follicles, each containing a primary oocyte (Figure 1). Only a small fraction of these oocytes will reach the correct maturation stage and acquire the potential to be released and fertilized. Oocytes and spermatozoa, the gametes, undergo a special kind of cell division called meiosis, which consists of two consecutive divisions, the end result being the reduction of the chromosome number to half. This means that, in the germline, a diploid human cell (46 chromosomes) eventually gives rise to four haploid cells (23 chromosomes each). During fertilization, each haploid gamete contributes half of the chromosome complement, thus generating a normal embryo. In a newborn, primary oocytes are paused at the beginning of the meiotic division (“meiotic arrest”), and remain so throughout childhood. Early stages of oocyte development include the germinal vesicle (GV) and metaphase I (MI) stages (Figure 2). Because these stages are part of the first meiotic division, the cell is still diploid and, therefore, it is still considered "immature". Once puberty is reached, a pituitary gonadotropin called follicle-stimulating hormone (FSH) promotes the growth of a cohort of follicles every month. But only those at the right stage of maturation will go on, along with their respective oocyte, which comes out of the arrest and resumes meiosis. By the time ovulation occurs, triggered by the surge of the luteinizing hormone (LH), oocytes have already completed the first of the two meiotic divisions, which means the primary oocyte has already divided into two cells: the first polar body and the secondary oocyte. The former is just a small cell that contains the corresponding chromosomes that result from the cell division. It never participates in embryogenesis, and so it has no genetic contribution to it. The latter in turn continues through the second meiotic division, until it arrests at MII (metaphase II) stage before ovulation (Figure 2). These oocytes (eggs) are considered mature, and they can be fertilized by sperm once ovulated. However, if fertilization does not occur, meiosis is never completed in the oocyte (2). MAIN ASPECTS NEEDED FOR THE EGG TO ACHIEVE FULL MATURATION Follicle growth and oocyte maturation are both influenced by circulating levels of gonadotropins (FSH and LH) and steroids (progesterone and oestrogens), among other factors. As parallel processes in time, they should accomplish certain events to ensure the formation of a fully mature egg by the time the follicle has acquired its maximum size ("Graafian follicle" = 18-21 mm) (3). Maturation status of the oocyte is defined by: 1. Nuclear maturation of the egg. This means the oocyte needs to reach a specific stage of meiotic division (MII stage), thus ensuring the appropriate chromosome number (genetic material) has been achieved (4). 2. Cytoplasmic maturation. In addition to the organization of the genetic material, the oocyte must complete a series of events such as distribution of mitochondria (the power source of the cell) or formation and relocation of the cortical granules (which will play a key role during fertilization), among others. This will guarantee the readiness of the egg for the sperm arrival (4). 3. Follicle maturation and growth. The follicle must increase its volume accordingly with the progression of the oocyte maturation; follicular cells are to be reorganized and differentiate into distinct layers to ensure blood supply and facilitate communication with the egg. Should any of these events fail to complete, fertilization will be greatly compromised (5).  Figure 2. Different stages of oocyte maturation. (A) Germinal vesicle (GV). The nucleus of the oocyte is still visible at an eccentric location (arrow), indicative of an early stage of meiosis. (B) Metaphase I (MI). The nuclear envelope has disorganized and the chromosomes (not seen) are preparing for division. No other evident features can be clearly distinguished under the optical microscope. (C) Metaphase II (MII). First division of meiosis has been completed, evidenced by the presence of the first polar body (arrow). The oocyte is now arrested at the second division; the nucleus is not distinguishable because chromosomes are again prepared for division, should fertilization happen. 400x magnification (original images modified from [6]). POSSIBLE CAUSES FOR FAILURE IN EGG MATURATION DURING ASSISTED REPRODUCTION TREATMENTS During assisted reproduction cycles, women are subjected to controlled ovarian hyperstimulation (COH) by the application of a variety of protocols in order to promote the growth of multiple follicles. One of the main actors used in these stimulation protocols is the human chorionic gonadotropin (hCG), which causes the oocyte to progress through meiosis and take over the role of LH in triggering ovulation (7). The use of conventional protocols allows most of the oocytes obtained to be at MII stage by the time of egg collection. However, some of these eggs could remain immature despite ovarian stimulation (8). Some estimations have suggested that around 20%-30% of collected oocytes do not achieve full maturation (9), although such figures may actually be higher as a consequence of the stimulation of multiple follicles. In some rare cases, it is possible to observe a phenomenon known as "oocyte maturation arrest", in which oocytes keep arrested during the maturation process, thus not being able to complete it. As a result, there is an increased number of collected oocytes actually arrested at either GV or MI stage (10). Explanations for these rare cases include several possibilities: 1. It could be due to failure in ovarian stimulation response. Both LH activity and hCG timing are directly related to the meiotic progression of oocytes, so the abnormal function of the hormone stimulation mechanisms may negatively impact clinical outcomes. In these cases, results might be improved by the modification of doses, hCG forms or stimulation protocols in successive cycles (11). 2. Specific follicular cells may present defective signalling mechanisms, which would result in abnormal response to gonadotropins and the subsequent inability of the egg to progress through meiosis (12,13). 3. Oocytes unable to reach a minimum size cannot progress further than GV or MI stage. In those cases, the growth of the follicle is limited, which means follicular cells do not acquire the ability to respond to gonadotrophic signals and promote maturation up to MII stage of the oocyte (13). 4. The acquisition of "meiotic competence" is controlled by the so-called maturation promoting factor (MPF). The activity of this molecular machinery may be compromised in certain patients suffering from rare heritable molecular defects. In such cases, the end result could be the inability of oocytes to reach the mature stage (14). In spite of these hypotheses, only a few cases of oocyte maturation failure in ART treatments have actually been reported (11). Additionally, the modification of hCG doses, in vitro maturation (IVM) of oocytes and intracytoplasmic injection of MPF seem to be the best options to date to overcome meiotic arrest (15). Even in the most difficult cases, egg donation may be a potential solution. The approaches mentioned above are just suggestions and theoretical solutions; this means further research is needed in order to improve our knowledge on the actual causes for oocyte maturation failure. Only by doing so will we be able to better deal with this situation. REFERENCES
5 Comments
|
Categories
All
 2016-2019. All Rights Reserved by Embryologist Media. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License . |
Embryologist Media
