|
“HIV+ serodiscordant couples should seek advice from fertility experts regarding the optimal route for safe conception” Author: Belén Gómez Giménez  CCO. Public Domain Human Immunodeficiency Virus (HIV) is a retrovirus that attacks and weakens the immune system (body's defense) against infections, diseases and some types of cancer. The most advanced stage of HIV infection is Acquired Immunodeficiency Syndrome (AIDS), which can take from 2 to 15 years to develop after infection (1). At least 36.9 million people have been estimated to be infected by HIV. In the past, patients were given short life expectancy but, due to the introduction of combined antiviral therapies, HIV is now classed as a chronic disease. Estimations from the World Health Organization (WHO) are that, between 2000 and 2017, the number of new infections and deaths were reduced by 36% and 38%, respectively. As a result, nowadays there are more HIV carriers who can enjoy a normal life, which allows them to pursue family planning. Nevertheless, certain risk of the virus transmission to both the offspring (vertical transmission) and the partner (horizontal transmission) is still to be considered (1). There is disagreement among experts on whether natural conception is safe in HIV+ couples or whether they should turn to assisted reproduction techniques (ART) instead. There is some evidence that virus transmission in seropositive couples with a highly active antiretroviral therapy (HAART), in combination with timed intercourse and pre-exposure prophylaxis for the HIV negative partner, is associated with minimal risk, thus allowing for natural conception. On the contrary, other studies recommend ART-based approaches, since these represent a safer choice for serodiscordant couples who have access to these modern methods (2). Female HIV-seropositive Non-coital ovulatory vaginal or intrauterine insemination (IUI) is a simple, safe method for infected individuals to get pregnant. In addition to this, patients should continue with HAART, which suppresses the viral load during the course of pregnancy and breast-feeding to minimize the risk of vertical transmission to the offspring (2). HIV-seropositive males Males can transmit the virus through seminal fluid and, as a result, partners and/or offspring may result infected. Semen induces changes in the female reproductive tract that promote conception and pregnancy. However, these alterations can also facilitate HIV activation, thus increasing the likelihood of the partner becoming infected with HIV (3). Human seminal plasma is a made up of a mix of fluid secretions, in which cell types other than sperm are found. These non-sperm cells have been recognized to be the agent behind viral transmission (4). Consequently, a method to overcome spreading of HIV known as “sperm washing” was developed, based on the principle of separating motile sperm from free HIV particles and infected cells (5). This method was first applied to sperm in 1992 (6). The sample protocol for working with HIV-seropositive semen samples in laboratories is summarized below (5, 7): In order to avoid viral contamination, it is necessary to work in isolated laboratories (biosafety cabin workstation, exclusive centrifuge) and set samples apart from non-infected samples when stored in nitrogen tanks to avoid cross-contamination. Otherwise, the same standard sperm preparation procedures are applied for infected and non-infected samples, as outlined as follows:
Depending on female characteristics such as age, reproductive tract malformations or endometriosis and male partner semen parameters, different methods of assisted reproduction may be applied. The simplest one is IUI, but in the presence of any limiting factors, either in vitro fertilization (IVF) or intracytoplasmic sperm injection (ICSI) is used. Differences between these procedures have been explained in our previous post. The main difference between non-infected and HIV+ sample preparation is that the latter requires the sperm washing procedure. This protocol entails two distinct preparation techniques (Figure 1): density gradient centrifugation (DGC) and swim up.
The consecutive use of these two techniques has achieved a notable reduction in the risk of transmission of the virus. 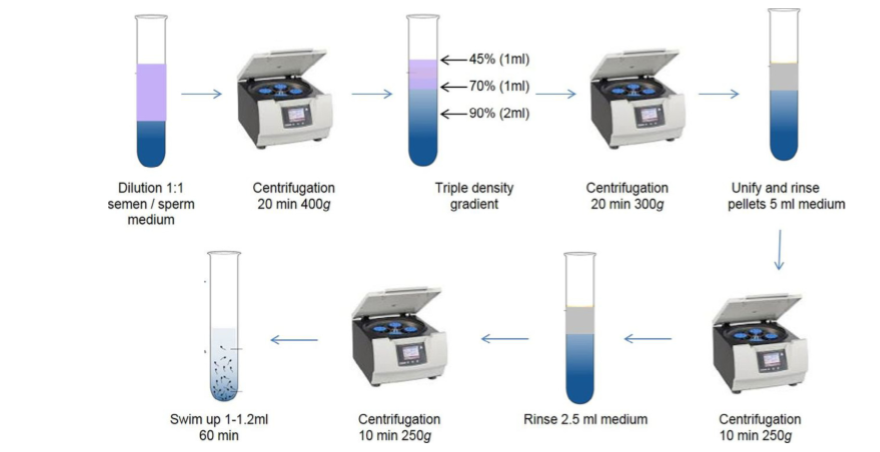 Figure 1: Semen washing procedure (9). Following sperm preparation, polymerase chain reaction (PCR) will be performed to analyse the genetic content of spermatozoa and screen for HIV. This technique, however, is limited by the fact that the analysed sperm only represent a small fraction of the overall sample, which can lead to a false negative result. CONCLUSIONS Semen washing is the best method to eliminate the presence of HIV in sperm and avoid transmitting the virus to the partner or offspring. Although there are studies that suggest that natural coitus can be a safe method if the patients are treated with anti-retroviral therapies, the general consensus is that this is not recommended if the affected couple has access to ART (2). Throughout ART treatment, pregnancy and during the first year after birth, diagnostic testing for both the mother and infant is recommended to ensure transmission has not occurred (5). Within assisted reproduction, there is no consensus on which method (IUI, IVF or ICSI) should be used in patients, and so this decision will be based on the HIV status of the couple (female positive, male positive or both), as well as their own fertility potential. Many studies have demonstrated that after semen wash, the risk of vertical and horizontal virus transmission is significantly reduced, showing that this is an effective procedure (10). Despite this, certain studies must be taken into account that have reported presence of the HIV-virus in spermatozoa following the procedure (11). Overall, it is critical that more studies are carried out to demonstrate these techniques are completely risk-free, and efforts should be made to unify the semen washing protocol between laboratories (10). HIV+ serodiscordant couples should always seek advice from fertility experts regarding the optimal route for safe conception. REFERENCES
1- WHO: HIV/AIDS [Internet]. Geneva: World Health Organization; c2018 [ cited 2018 August 31]. Available from: http://www.who.int/en/news-room/fact-sheets/detail/hiv-aids. 2- Zakarin Safier L, Sauer MV. Fertility care interventions should be provided as the first line options for HIV+ serodiscordant couples who desire children in settings with affordable access to care, regardless of their fertility status. J Int AIDS Soc. 2017;20(Suppl 1):21294. 3- Doncel GF, Anderson S, Zalenskaya I. Role of semen in modulating the female genital tract microenvironment--implications for HIV transmission. Am J Reprod Immunol. 2014;71(6):564-74. 4-Jindal SK, Rawlins RG, Muller CH, Drobnis EZ. Guidelines for risk reduction when handling gametes from infectious patients seeking assisted reproductive technologies. Reprod Biomed Online. 2016;33(2):121-30. 5-Medicine PCoASfR. Recommendations for reducing the risk of viral transmission during fertility treatment with the use of autologous gametes: a committee opinion. Fertil Steril. 2013;99(2):340-6. 6- Semprini AE, Levi-Setti P, Bozzo M, Ravizza M, Taglioretti A, Sulpizio P, et al. Insemination of HIV-negative women with processed semen of HIV-positive partners. Lancet. 1992;340(8831):1317-9. 7- Garrido N, Meseguer M, Bellver J, Remohí J, Simón C, Pellicer A. Report of the results of a 2 year programme of sperm wash and ICSI treatment for human immunodeficiency virus and hepatitis C virus serodiscordant couples. Hum Reprod. 2004;19(11):2581-6. 8- WHO laboratory manual for the examination and processing of human semen- 5th ed. In: Geneva: WHO Press, 2010. 9- Zamora MJ, Obradors A, Woodward B, Vernaeve V, Vassena R. Semen residual viral load and reproductive outcomes in HIV-infected men undergoing ICSI after extended semen preparation. Reprod Biomed Online. 2016;32(6):584-90. 10- Mencaglia L, Falcone P, Lentini GM, Consigli S, Pisoni M, Lofiego V, et al. ICSI for treatment of human immunodeficiency virus and hepatitis C virus-serodiscordant couples with infected male partner. Hum Reprod. 2005;20(8):2242-6. 11- Elizaveta E B, Bocharova E, Azova M. Spermatozoon as a Vehicle for Viruses. Int J cell Sci & mol biol. 2017; 2(4) : 555593.
0 Comments
|
Categories
All
 2016-2019. All Rights Reserved by Embryologist Media. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License . |
Embryologist Media
