|
"Chromosome organization has been proposed to have potential functional implications in male fertility". Author: Lidón Carretero Vilarroig 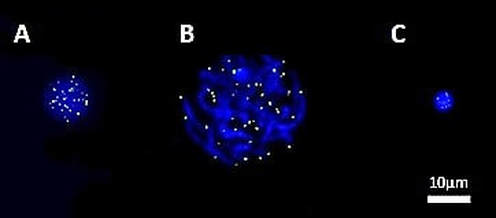 Fig. 1. FISH-PNA telomere signals (green) on different stages of sperm maturation (genetic material stained in blue): (A) spermatogonium; (B) primary spermatocyte; (C) sperm cell [in collaboration with CIMAB (Centro de Infertilidad Masculina y Análisis de Barcelona, Spain)]. WHAT ARE TELOMERES? Telomeres are nucleoprotein complexes located at both ends of linear chromosomes. In the case of vertebrates, there are hundreds of tandem repeats of the sequence TTAGGG. Together with their protein complex, telomeres play a very important role in stability and replication of chromosomes, preventing their breakage and regulating recombination between homologs (1, 2). Telomere length (TL) is determined by various loci located on several autosomes and on the X chromosome. In addition, factors such as age, gender and free radical levels have an effect on TL, as well as specifically the age of the father at the time of conception of the offspring (3). Meyerson et al estimated that the mean TL varies between 5 and 10 kb in somatic cells, and between 10 and 20 kb in germ cells, depending on the species and cell type studied (4). However, in somatic cells telomeres suffer from shortening in each round of replication; this is due to the inability of the DNA polymerase, the enzyme in charge of synthesising DNA, to elongate the 5’ end (known as “End Replication Problem”) (5). By contrast, germ cells count on an active enzyme able to solve this problem: the telomerase. Nevertheless, this enzyme is only active in specific cell lines, stem cells and immortal cancer cells. TELOMERES IN SPERM CELLS Telomeres play a main role in the organization of chromosomes inside the nucleus of sperm cells, since they take up specific non-random positions (6, 7) (Fig. 2). Although different models have been proposed to explain chromosome organization inside the sperm nucleus, it is well accepted the idea that every chromosome has a particular position, known as chromosome territory (Fig. 2) (7). Some authors have described a dynamic length during spermatogenesis: telomeres shorten during the early stages of sperm differentiation, whereas by the end of the process they elongate again, even exceeding their starting length (8). It is also known the importance of telomeres in chromosome recognition during cell division. They regulate recombination of homologous chromosomes and seem to be the first structure from the paternal nuclear genome to respond to signals after fertilization, leading to pronucleus formation (1, 2). 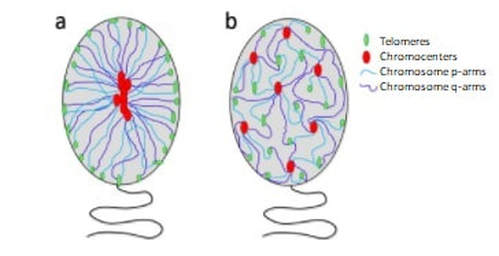 Fig. 2. Schematic representation of the proposed models of chromatin organization within sperm nuclei (7). SPERM CELL TELOMERES AND MALE INFERTILITY Telomeres have been targeted as potential candidates to explain some cases of infertility, since they are one of the epigenetic regulatory mechanisms required for proper embryogenesis (9). Due to the fact that telomeres are directly involved in chromosome recognition during cell division, modifications in the structure and length of telomeres may be related to abnormal chromosomal dotation (10). Shorter telomeres in spermatozoa may be a leading cause of aneuploidy (11), being this related to recurrent pregnancy loss. The proper organization and length of telomeres contribute to an accurate cell division, thus generating sperm cells with the right chromosome complement. Regarding their arrangement inside the nucleus, chromosome territories are thought to be organized in such a way that they allow for the actual interaction between genes from different chromosomes. Given the importance of such interactions, chromosome organization has been proposed to have potential functional implications in male fertility. Alterations in TL have been previously studied, suggesting a link between telomere shortening and errors during programmed cell death (apoptosis), sperm maturation and reduction in fertility (12, 13, 14). Also, DNA damage has been associated with disruption of the normal telomere–telomere interactions, leading to possible loss of the typical loop configuration of telomeres found in chromosomes. This would imply abnormalities in sperm chromosome deposition, activation and processing by the oocyte at the time of fertilization (15). Several studies in mice have suggested the existence of a protective mechanism that would degrade spermatocytes with reduced telomere length to prevent their maturation. Should this checkpoint fail, defective spermatocytes with shortened telomeres would be able to progress through meiosis (the typical division of gamete precursors) (16, 17), thus resulting in potentially abnormal (non-functional) sperm cells. CONCLUSIONS Telomere length could be one of the causes to explain some cases of male infertility of unknown origin. Some authors have described shortened telomeres from both sperm and ova to have additive effect on limiting the potential growth of embryos. Despite all these considerations, the actual role of telomere length in male infertility remains to be further investigated. REFERENCES 1. Ozturk, S. Telomerase Activity and Telomere Length in Male Germ Cells. Biol. Reprod. 92, 53–53 (2015). 2. Bekaert, S., Derradji, H. & Baatout, S. Telomere biology in mammalian germ cells and during development. Dev. Biol. 274, 15–30 (2004). 3. Thilagavathi, J., Venkatesh, S. & Dada, R. Telomere length in reproduction. Andrologia 45, 289–304 (2013). 4. Meyerson, M. Role of telomerase in normal and cancer cells. J Clin Oncol 18, 2626–2634 (2000). 5. Rieko Ohki, Toshiki Tsurimoto and Fuyuki Ishikawa. In Vitro Reconstitution of the End Replication Problem. Molecular and cellular biology 2001 Sept. 2001, p. 5753–5766 6. Mudrak, O., Tomilin, N. & Zalensky, A. Chromosome architecture in the decondensing human sperm nucleus. J. Cell Sci. 118, 4541–4550 (2005). 7. Ioannou, Dimitrios; Millan, Nicole M.; Jordan, Elizabeth; Tempest, Helen G. A new model of sperm nuclear architecture following assessment of the organization of centromeres and telomeres in three-dimensions. Scientific Reports. 2017/01/31/online VOL7; 41585 http://dx.doi.org/10.1038/srep41585 10.1038/srep41585 8. Tanemura, K. et al. Dynamic rearrangement of telomeres during spermatogenesis in mice. Dev. Biol. 281, 196–207 (2005). 9. Esteves SC. A clinical appraisal of the genetic basis in unexplained male infertility. Journal of Human Reproductive Sciences. 2013;6(3):176-182. doi:10.4103/0974-1208.121419. 10. Hanna, C. W. et al. Telomere length and reproductive aging. Hum. Reprod. 24, 1206–11 (2009). 11. Treff, N. R., Su, J., Taylor, D. & Scott, R. T. Telomere DNA deficiency is associated with development of human embryonic aneuploidy. PLoS Genet. 7,e1002161 (2011). 12. Fujisawa, M. et al. Telomerase activity in the testis of infertile patients with selected causes. Hum. Reprod. 13, 1476–9 (1998). 13. Cheng, E.-H. et al. Evaluation of telomere length in cumulus cells as a potential biomarker of oocyte and embryo quality. Hum. Reprod. 28, 929–36 (2013). 14. Moskovtsev, S. I., Willis, J., White, J. & Mullen, J. B. M. Disruption of telomere-telomere interactions associated with DNA damage in human spermatozoa. Syst. Biol. Reprod. Med. 56, 407–12 (2010). 15. Disruption of Telomere–Telomere Interactions Associated with DNA Damage in Human Spermatozoa. Sergey I. Moskovtsev, Jennifer Willis, John White & J. Brendan M. Mullen. Systems Biology in Reproductive Medicine Vol. 56 , Iss. 6,2010 16. Hemann MT, Rudolph KL, Strong MA, DePinho RA, Chin L, Greider CW. Telomere dysfunction triggers developmentally regulated germ cell apoptosis. Mol Biol Cell. 2001;12:2023–30. 17. Liu L, Blasco M, Trimarchi J, Keefe D. An essential role for functional telomeres in mouse germ cells during fertilization and early development. Dev Biol. 2002;249:74–84.
4 Comments
"You should take your time to consider all ethical issues you may encounter within the process". Author: Sara Sanz 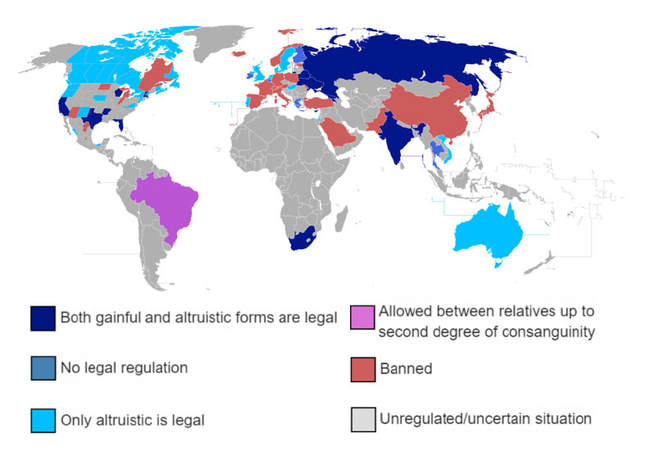 Fig 1. Current legal status of surrogacy around the world (1). The latest advances in assisted reproduction technologies have managed to make incredible things come true. Current advances are changing the lives of millions of people, giving them the opportunity to form their own family. One of the options that have opened new possibilities for parenthood is surrogacy. Perhaps, this is not as common as others, but it certainly hits the media every now and then. However, what have you heard about it? The following points are the main aspects everyone should know about this option: A) Who may need surrogacy. Prospective parents are individuals who seek a surrogate mother because: 1. There is actually a medical condition that makes it impossible or dangerous for the woman to get pregnant and/or to enter labour. 2. He is a single man who wants to become a father (2). 3. They are a gay men couple who want to form a family with a genetic link (3). B) Who is the surrogate mother, and how does the entire process usually take place? The surrogate mother is a woman who carries out a pregnancy as a donation in order to help form a new life. This process can take place with or without her own eggs. If it is her eggs that are used, the process is referred to as traditional surrogacy; otherwise, it is called full or gestational surrogacy. If this is the case, embryos can be derived from three different sources (4): 1. Eggs and sperm that belong to the intended parents. 2. Donor eggs fertilized by the sperm of the intended father. 3. Both eggs and sperm obtained from donors. C) Whether surrogacy entails remuneration depends on the country. If the surrogate mother does not receive a payment (although prospective parents may provide reimbursement for medical care), the arrangement is known as non-commercial surrogacy, which is common between family members or friends. On the contrary, if the surrogate mother does receive compensation, the term used for the arrangement is commercial surrogacy (5). D) Where this procedure may be carried out depending on local regulations. As shown above (Fig. 1), surrogacy is only allowed in certain countries, each one with its own legal regulations. For instance, some of them only permit the altruistic form, in others surrogacy is available just for resident citizens, and in some others this option is only allowed for heterosexual couples. Therefore, it is essential to know which country/countries present the appropriate legislation in each particular case, reason why before choosing a destination it is important to find out some key aspects, such as (6):
E) Perhaps the first question to ask actually is: "does this option feel right for me? Every single person and situation are unique, and so you may end up wondering whether this is the right path to form your family. Regarding such a delicate topic you should first question yourself, and carefully take your time to consider all ethical issues you may encounter within the process. It is important to consider that there exist multiple support groups and agencies that can help you resolve all your technical and ethical doubts with respect to this process. Therefore, it is advisable to first gather all available information in order to answer every question. Only then would it be safe to achieve your dream of starting a family the way you decide. REFERENCES 1. Surrogacy. In: Wikipedia [Internet]. 2017. Available from: https://en.wikipedia.org/w/index.php?title=Surrogacy&oldid=810900302. 2. Carone N, Baiocco R, Lingiardi V. Single fathers by choice using surrogacy: why men decide to have a child as a single parent. Hum Reprod Oxf Engl. 2017 Sep 1;32(9):1871–9. 3. Blake L, Carone N, Raffanello E, Slutsky J, Ehrhardt AA, Golombok S. Gay fathers’ motivations for and feelings about surrogacy as a path to parenthood. Hum Reprod Oxf Engl. 2017 01;32(4):860–7. 4. Humbyrd C. Fair trade international surrogacy. Dev World Bioeth. 2009 Dec;9(3):111–8. 5. Raposo VL. The new Portuguese law on surrogacy - The story of how a promising law does not really regulate surrogacy arrangements. JBRA Assist Reprod. 2017 Sep 1;21(3):230–9. 6. Families through Surrogacy. Available from: http://www.familiesthrusurrogacy.com/ "A series of different factors in lifestyle can be altered in order to enhance the overall welfare (...) they play a key role in determining our reproductive health (...)". Author: Noemi Díaz Arróniz  Photo by Mon Petit Chou Photography on Unsplash Infertility is considered a clinical condition, defined (by consensus) by the failure to achieve natural pregnancy after one year of unprotected sexual intercourse (1). It implies serious psychological consequences, and so it results in a stressful experience for infertile couples (2). The prevalence of infertility has increased since 1955, and nowadays it affects at least 15% of couples in reproductive age (1, 2). A series of different factors in lifestyle can be altered in order to enhance the overall welfare. It is important to remember that these factors are ultimately under our own control, because they play a key role in determining our reproductive health and they can positively or negatively affect fertility (1). The concept "quality of life" (QOL) refers to the well-being of individuals, and it is affected by both individual and social factors (3). Here we report the potential effects of different lifestyle factors on the reproductive health of men and women. Even though many aspects of life are not subjected to modification, lifestyle itself may be changed for good (1). 1. TIMELINE OF REPRODUCTION: ADVANCED AGE. Advanced maternal age is a risk factor for fertility, and it has been reported to be directly related to a variety of problems, such as pregnancy loss, obstetric complications, foetal anomalies and different genetic conditions like Down syndrome. Due to changes in lifestyle, economic factors, social environment, or the will to grow professionally and acquire a proper education level, numerous couples currently choose to delay their parenthood. This implies that the age to father children becomes slowly (but inevitably) higher (1). Advanced age negatively influences the clinical pregnancy rate after in vitro fertilization (IVF). In particular, this responds to an increased rate of embryo aneuploidies. Several studies have shown a direct relationship between the risk of foetal loss and the age of women older than 35 (5). 2. STRESS It is of no surprise that the current rhythm and lifestyle generates high levels of anxiety, and alterations of the endocrine system can seriously affect fertility (1). Both folliculogenesis and spermatogenesis (production of eggs in the ovaries and sperm in the testes, respectively) are strictly regulated by several hormones, and so any alteration of the hormone balance may have immediate negative effects on the quality of eggs and/or semen (5). It is also worth remembering that the stress caused by the frustration of not achieving pregnancy can directly affect hormone levels and, consequently, impede conception in first place (1). 3. NUTRITION Taking care of nutrition habits is essential not only for the overall health, but also for reproductive health (7). A balanced diet can help to improve fertility and reproductive potential for both men and women. The lack of specific elements or nutrients may eventually derive in some degree of infertility (2). As an example, it is always recommended to have a regular intake of food rich in antioxidants, such as fruit, vegetables, fibre, carotenoids.... (1). Besides containing antioxidants and essential nutrients, vitamins and folate are found in fruit and vegetables; these substances are involved in DNA and RNA synthesis, and thus play an important role in spermatogenesis by protecting the sperm DNA from free radical damage (7). Modifying dietary habits can affect ovarian function, which can be correlated with changes in the concentration of circulating hormones including insulin and leptin. These hormones are tightly associated with the initiation and synchronisation of follicle growth, and it seems that its production is regulated, at least partially, by oestrogen secreted by the developing follicle. It is also advisable to minimise the intake of saturated fats and cholesterol, to avoid excess that might affect the production and balance of sexual steroid hormones like progesterone. Insulin and leptin, in turn, are also associated with the proper initiation of menses; young girls with the wrong levels of certain hormones may see their menarche delayed or even suppressed. Maintaining a healthy body weight is also essential for the optimal reproductive potential. A reduced index of body fat may impede the regular ovarian cycle in women. Also, obesity is one of the factors with a high impact on fertility, and one of the main causes of adverse effects on the early development of the embryo, too. Numerous studies have demonstrated a direct relationship between excess body mass and the diminished reproductive capacity (1). On one hand, obesity increases the probability of suffering from miscarriage due to endocrine and metabolic alterations. It affects the quality of eggs and, subsequently, the embryos formed after fertilization (which may also result in severe developmental problems for the neonates). And on the other hand, an excessively low body mass index (BMI) also reduces the chances of pregnancy due to hormone imbalance and the inability to produce specific sexual hormones, which in turn cause abnormal menstrual cycles and obstetric complications (7). 4. TOBACCO AND ALCOHOL The ingestion of toxic substances like tobacco, alcohol and other drugs has a potentially harmful effect on both oocytes and sperm. In men, consumption of alcohol has been linked with several negative side effects, such as testicular atrophy, decreased libido and reduced sperm count (1, 2). These symptoms are also typically found on those men who present steroid abuse (like in some cases of bodybuilders) (8). Alcohol use during pregnancy is an established cause of foetal alcohol syndrome (FAS). Several studies have recommended that pregnant women should avoid alcohol during pregnancy. In recent years it has consistently been shown that one drink (or more) per day or more increases the risk of spontaneous abortion, intrauterine growth retardation and low birth weight. An increased alcohol intake intake may reduce birth length and head circumference, cause preterm birth, defects in development and cognitive problems (9). Nicotine abuse, in turn, may impede sperm motility and affect their overall viability. But high consumption of tobacco may also cause genetic alteration in ovocytes and, therefore, in embryos derived from them (2). Women seeking to get pregnant are normally limited their coffee intake up to no more than 2-3 cups per day. Again, the abuse of caffeine may result in higher probabilities of suffering from a miscarriage (2, 8). 5. ENVIRONMENTAL FACTORS Exposure to certain chemical substances like pesticides or simply heavy metals may disturb the hormonal balance and negatively impact fertility. This is particularly evident in men; modern lifestyle features including pollution, large urban areas or industry have left their impact on the capacity of producing sperm within the last decades (2). For instance, direct and continued exposure to heat sources or radiation have a direct effect on sperm DNA fragmentation and motility, which are some of the main features to be assessed in semen analyses. Not surprisingly, the reduced quality of sperm has been documented in men having close and long exposure to mobile devices like laptops and even ovens or saunas (7). 6. PHYSICAL EXERCISE The regular practice of sports and moderate intensity exercise is beneficial and helpful when it comes to maintain a healthy weight, but also to reduce the levels of stress and anxiety (6). Men who exercise at least three times a week for one hour have been reported to score higher in almost all sperm parameters, compared to men who participated in a more frequent and intense physical activity (1). Also, and as it has been previously mentioned, the regular consumption of anabolic steroids is an important cause of male infertility, due to the hampered action of testosterone in the testes (1, 7). CONCLUSIONS Modern lifestyle has been shown to play an important role in fertility. Attempting pregnancy before the age of 30-35 may provide the highest probabilities of success for women. Considering social, professional and personal reasons, it is then advisable to take into account the current possibilities available for fertility preservation while still possible (1). Because of the impact of nutrition and physical activity on fertility, controlling and maintaining healthy dietary habits (as well as a healthy weight) may provide a way for couples to increase their chances to conceive (1). As long as there is no pathological cause for infertility, the solution to some related problems may be as simple as to correct certain wrong habits (8). By understanding the impact of lifestyle on reproductive health and by actively modifying specific behaviour patterns, men and women may be capable of controlling their own fertility potential (1). REFERENCES
http://www.who.int/reproductivehealth/topics/infertility/definitions/en/ (september 5, 2017) http://www.minifiv.es/2017/02/como-afecta-el-estilo-de-vida-a-la-fertilidad/ (september 20, 2017) Author: Belén Gómez Giménez  CCO. Public Domain It is well known that women age is important for reproduction. The female biological clock is well-defined temporally and biologically, with declining oocyte production when the woman is in her late 30s or early 40s and cessation of menses in the late 40s and early 50s. Whereas woman’s chances to conceive naturally drop sharply, male fertility does not cease abruptly, since androgen production and spermatogenesis continue throughout life. There are some worldwide-known examples of famous personalities who fathered children at an advanced age, like Julio Iglesias´s senior (90), Luciano Pavarotti (68) or Rod Stewart (66). A great problem in our society and that of industrialized countries is that couples wait longer to have children, and advances in reproductive technology currently allow older men and women to consider being parents. However, many studies highlight age as an important factor to conceive in both sexes. During years, fertility research has focused mainly on women age, and so potential adverse effects of male age might have passed unnoticed. However, there is currently a great concern about the decreasing quality of sperm with age in men. In 2010, the World Health OrganiSation (WHO) changed criteria to semen evaluation, due to a decreased concentration and normal sperm morphology below the threshold for which a semen sample was considered of good quality. 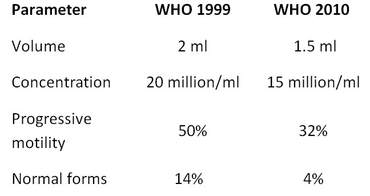 Table 1: Changes in seminal quality assessment criteria (9), (10). On the other hand, some research lines show that in men, advanced age affects sperm quality (decreases semen volume and reduces the percentage of normal sperm morphology and motility). It also affects non-reproductive physiological issues such as libido or erectile function. Blood testosterone levels decline with age in most men, even in healthy ones; this decline probably begins around the age of thirty, which has been termed andropause. So, similarly to women, aging in men is also associated to a drop in sex hormone levels; therefore, we can talk about an effective male biological clock. These changes in sex hormone levels and sperm quality could affect fertility, because sperm genetic material is altered and, as a consequence, the risk of spontaneous abortion is increased due to offspring genetic abnormalities. IS AGE IN MEN ASSOCIATED WITH DIFFERENT OFFSPRING DISEASES OR LIVE BIRTH RATES? These alterations could explain the association of paternal age with the increased incidence of some psychiatric disorders such as those of the autism spectrum, psychosis, schizophrenia and bipolar disorders at childbearing. Moreover, there seems to be supporting evidence that paternal age significantly influences the incidence of having a child with Down syndrome when combined with maternal age. This could also be the case for other genetic abnormalities, which could in turn lead to miscarriage or different diseases in the newborns. Finally, It has been demonstrated that men over 35 years old are twice as likely to be infertile (defined as the inability to achieve a pregnancy within 12 months). 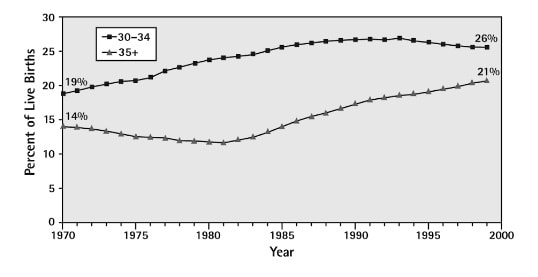 Figure 1: Percentage of live births by age of father (4). A recent study reported at European Society of Human Reproduction and Embryology congress in July 2017 found that couples with both members under 30 had around 70% chance of having a live birth after an in vitro fertilization cycle. However, that success rate fell to around 50% when the man was aged 40-42. CONCLUSIONS In summary, age is an important factor both in women and in men, but It should also be taken into consideration that there are other factors such as obesity, habitual alcohol and/or tobacco intake and stress, among other well-studied elements, which might be effectively altering our fertility potential. Currently available data not only show that male biological clock does exist, but it is also important to fertility. Mechanisms of action are unclear, but as above-exposed, they might involve impaired semen parameters and increased levels of damaged sperm DNA, which could affect fertilization, implantation and even embryo development. REFERENCES
1- D'Onofrio BM, Rickert ME, Frans E, Kuja-Halkola R, Almqvist C, Sjölander A, et al. Paternal age at childbearing and offspring psychiatric and academic morbidity. JAMA Psychiatry. 2014;71(4):432-8. 2- Dodge L, Penzias A, Hacker M. The impact of male partner age on cumulative incidence of live birth following in vitro fertilization. Oral communication at the ESHRE. 2017. 3- Eskenazi B, Wyrobek AJ, Sloter E, Kidd SA, Moore L, Young S, et al. The association of age and semen quality in healthy men. Hum Reprod. 2003;18(2):447-54. 4- Fisch, H. The male biological clock. In: D. Carrell, ed. Paternal Influences on Human Reproductive Success. New York: Cambridge University Press, 2013. pp.61-69. 5- Fisch, H, Braun S. In: Simon and Schuster, ed. The male biological clock. The startling news about aging, sexuality, and fertility in man. New York: Free press, 2005. p.10. 6- Fisch H, Hyun G, Golden R, Hensle TW, Olsson CA, Liberson GL. The influence of paternal age on down syndrome. J Urol. 2003;169(6):2275-8. 7- Harris ID, Fronczak C, Roth L, Meacham RB. Fertility and the aging male. Rev Urol. 2011;13(4):e184-90. 8- Pasqualotto FF, Borges Júnior E, Pasqualotto EB. The male biological clock is ticking: a review of the literature. Sao Paulo Med J. 2008;126(3):197-201. 9- WHO laboratory manual for the examination and processing of human semen- 5th ed. In: Geneva: WHO Press, 2010. 10- WHO laboratory manual for the examination of human semen and sperm-cervical mucus interaction- 4th ed. In: Cambrige University Press, 1999. Author: Shuyana Deba  Source: https://www.thebump.com/a/egg-freezing-three-women-tell-why-they-chose-to-do-it In today's society, egg freezing has become a trending issue, normally associated with those women who want to delay their maternity. But, what does egg freezing really mean? Let’s try to explain this item clearly from the point of view of the assisted reproduction laboratory. Oocyte cryopreservation is the term used for what is socially known as "egg freezing". Cryopreservation is an option for those who want to preserve their fertility. This process refers to the use of ultra low temperatures to preserve gametes (oocytes from women and spermatozoa from men). It can also be used to preserve embryos or even reproductive tissues (like ovarian or testicular tissue) down to subzero temperatures in order to stop all biological activity, maintaining the appropriate conditions for future use. This has been proofed of particular help in cases in which the individual had to be treated with aggressive therapies, like those required to fight cancer. In such cases, normally partial extraction of the gonadal tissue (ovary or testis) is followed by cryopreservation until the patient overcomes the clinical situation and is ready to conceive. After extensive research, most assisted reproduction laboratories currently use vitrification, an ultra rapid freezing technology (-196˚C with liquid nitrogen) that avoids the formation of damaging ice crystals in the cells while ensuring their viability after thawing for future fertilization. INDICATIONS FOR OOCYTE CRYOPRESERVATION This technique was initially reserved for those women with specific medical indications who had no other fertility options. Progress made in the field of cancer treatments has contributed to the increase of cancer survival rates in populations. However, these treatments are known to affect negatively the fertility potential. In those cases, oocyte cryopreservation can provide hope for fertility preservation. Egg freezing is also indicated for cases of premature menopause and, consequently, the loss of ovarian function at an early age. However, it must be considered that some cases of early loss of ovarian function might be due to genetic causes, which may be eventually transmitted to the next generation. That is why every single case must be addressed individually and independently subjected to counselling. This would allow to evaluate whether cryopreservation of oocytes and delayed motherhood is actually a good option. Nowadays, another application for oocyte vitrification is the creation of donor oocyte banks for egg donation programs. One of the great advantages of this is that menstrual synchronization between donor and recipient is not required. Moreover, leftover oocytes are stored for another cycle. Furthermore, oocyte cryopreservation is useful in those cases in which the woman has been subjected to ovarian stimulation, and yet the male partner fails to produce a semen sample on the day of oocyte recovery. Additionally, it has also been proposed as an efficient strategy for women who had a low response to the stimulation treatments, so the oocyte number recovered in a cycle is not high enough. Thanks to vitrification, those women can store and accumulate oocytes from multiple ovarian stimulation cycles. However, as it has been mentioned above, the egg freezing approach is currently catching more attention from society due to the increasing number of women who want to delay their motherhood. This means they would be attempting to preserve fertility ahead of any age-related issue that could decrease it. The reason is that fecundity in women is gradually reduced, but there is a significant decline around age 32, and even more pronounced from 37 onwards. This scientific fact is explained by the natural reduction of the oocyte number in the ovaries (ovarian reserve), which happens naturally and progressively in every healthy woman. So, age at the time of oocyte cryopreservation is crucial for the outcome of the technique. It is also worth to take into consideration the number of embryos generated during cycles. Since implantation rates have improved considerably and the risks of multiple pregnancy are high, there is a tendency to perform single embryo transfer, when possible. Due to the controversy around the definition of an embryo (meaning legal definition that refers to legal rights of the unborn), cryopreservation of supernumerary embryos have raised ethical and legal concerns in many countries. As a consequence, it is not uncommon to see differences in legislation on these matters between countries. With this regard, cryopreservation of oocytes can bypass such problems, given the fact that an oocyte is by no means an individual or human being when it comes to legal issues. FACTORS AFFECTING OOCYTE SURVIVAL The main difficulty the oocyte faces for cryopreservation is its own shape and volume. In particular, the oocyte membrane gets frequently damaged and ruptured, which could lead to immediate death of the cell. Since the oocyte is a single cell structure, there is no backup for recovery from serious injuries, as opposed to multicellular embryos. Additionally, women age at the moment of egg freezing is a critical factor, not only because the oocyte number decreases over time, but also because their quality is reduced, as well. In fact, several clinical studies have shown that oocyte survival after cryopreservation is higher in younger women (<35 years old) than in +36-year old women. RESULTS OBTAINED USING VITRIFIED OOCYTES Several studies have demonstrated that there has been no increase in the number of anomalies in children born from oocytes fertilized after freezing and thawing. Nevertheless, the live birth rate per patient was statistically higher in younger patients compared to older ones (50% vs. 22.9%), regarding age at egg vitrification. Additionally, when older women go back to their vitrified oocytes, they are also more likely to experience pregnancy complications. It is important to highlight that society is not yet aware of the importance of age for oocyte vitrification. As a consequence, and even though elective freezing of oocytes for delaying childbearing is becoming one of the most frequent indications for fertility preservation, it is still a decision made at a late stage, after which results may not be as good as expected. It seems that there is not enough information for women on risks, potential, resources and outcomes. Given the tendency of today’s society to postpone the moment of childbearing, women should be aware of all possibilities and difficulties, the earlier the better. If science and media manage to spread that information so that it reaches young women at the right time, decision-making would be improved and women considering going for oocyte cryopreservation would be able to make up their mind on time before it is too late. REFERENCES
Authors: Inés Abad, Shuyana Deba and Javier Del Río  Sources: https://dietistaromeoluana.wordpress.com/2014/05/02/maternita-in-sovrappeso-piu-a-rischio-con-leta-avanzata/ WHAT IS OBESITY AND HOW DOES IT AFFECT FERTILITY? Obesity is an increasing epidemic disease in the industrialized world due to changes in lifestyle, reduced exercise and dietary habits. Other factors such as endocrine, hormonal or physiological disorders may lead to this disease. Nowadays, the World Health Organisation has described obesity as a body mass index (BMI) over 30 Kg/m2 and it is associated with cardiovascular disease, diabetes, osteoarthritis and malignancies such as endometrial or colon cancer. Also, this disease is currently listed as one of the causes of infertility in women. But, why obese patients tend to find more difficulties to get pregnant, both for natural and artificial conception? Numerous studies have described a delay in natural conception in obese women, mainly due to an increased risk of anovulation. However, even in obese women with regular cycles, it has been observed that the probability of pregnancy accumulated over a year is reduced by 5% for each unit of BMI that exceeds 30 kg/m2. These findings could suggest the absence of oocytes in spite of the existence of regular menstruations, the release of oocytes of low quality with a reduced potential of fertilization or the alteration of the endometrium. NEGATIVE IMPACT OF OBESITY ON WOMEN'S FERTILITY AND ASSISTED REPRODUCTION Scientific research has demonstrated that hormones found in gut and fatty tissue have an important role in the regulation of reproductive function. In cases of high caloric intake, which increases the fatty tissue, the level of those hormones is higher, interfering negatively in the hormone cascade that controls reproductive functions. Obese women’s hormones are out of balance and cysts are formed in the ovaries, leading to polycystic ovary syndrome. Consequently, women suffer from menstrual irregularity, hirsutism (excessive hair growth) and infertility. They also present higher probability of developing further affections such as diabetes or heart disease than average women. Moreover, when a woman is stimulated in order to obtain oocytes, the treatment to be applied is directly related to her weight. In women suffering from morbid obesity (BMI over 40 kg/m2), the dose of hormones to be administered needs to be significantly increased and, consequently, the risk of suffering from possible adverse effects such as ovarian hyperstimulation syndrome is also higher. Thus, this risk is especially important in obese women with polycystic ovaries, where the chances of achieving pregnancy through assisted reproductive techniques are significantly reduced. Consequently, female obesity is associated with fewer follicles, defective or reduced oocytes and embryos and lower live birth rates. Oocytes from overweight women present specific defects on metabolic pathways, which implies potentially impaired development of children, compared to those from women of BMI within the healthy range. These oocytes from overweight and obese women are smaller and less likely to reach the blastocyst (stage of development at which embryo undergoes implantation in the endometrium). However, those that manage to do so normally show accelerated preimplantation development and the subsequent blastocysts contain fewer cells, notably in the trophectoderm (the structures that will give rise to extra embryonic tissues and placenta). PREGNANCY IN OBESE WOMEN Obesity during pregnancy has short- and long-term adverse consequences for both mother and child. In early gestation, maternal obesity significantly increases the risk of complications, such as hypertensive disorders, gestational diabetes, preterm delivery, respiratory diseases or thromboembolic complications. It might cause spontaneous pregnancy loss and congenital anomalies. Metabolically, obese women have increased insulin resistance in early pregnancy, which is clinically manifested in late gestation as glucose intolerance and foetal overgrowth. At the end of pregnancy, the risk of cesarean delivery and complications at labour is greater in obese women. In addition, the altered metabolism of the embryo can be the cause of an overweight child at birth. DOES OBESITY HAVE AN IMPACT ON MEN'S FERTILITY? In men, obesity also has negative repercussions on their fertility. It has been suggested a relationship between the increase in BMI and the decrease of the concentration and mobility of their spermatozoa. This could be explained by the increase in fat tissue, which causes an imbalance of testosterone, one of the main hormones that play important roles in the maturation of spermatozoa. In addition, obesity can also lead to cardiovascular complications, diabetes or joint problems that are related to a decrease of semen volume and altered sperm DNA. These negative DNA changes may be related to lower pregnancy rates and increased risk of miscarriage, and can also lead to some serious birth defects. WHAT SHOULD I DO? Since there is evidence enough to affirm hat overweight influences fertility and fertility treatments, it is important to monitor health to avoid problems in general, and in particular those which may affect conception. If you have trouble conceiving it is always good to seek professional help and consult a specialist. REFERENCES
|
Categories
All
 2016-2019. All Rights Reserved by Embryologist Media. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License . |
Embryologist Media
