|
Author: María Caballero "(..) it is important to choose the appropiate fertility preservation procedure according to the treatment". 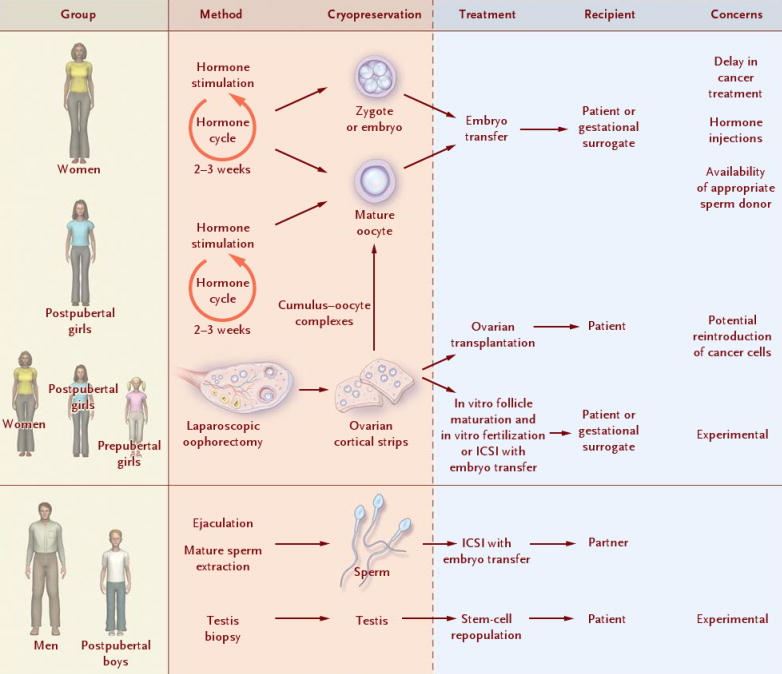 Figure 1. Fertility preservation procedures at prepubertal and adult age for both male and female individuals (1). Once someone is diagnosed with any kind of disease, the first step is to decide the appropriate treatment. In many cases, such treatment can seriously affect the reproductive capacity, and so it is important to consider the option of fertility preservation (FP) when it comes to individuals at reproductive age or prepubertal children (2, 3) (Figure 1). Although most of the articles about FP are related to oncology patients (4, 5, 6, 7), there are other diseases and situations in which considering FP may be also important. Some of these diseases include autoimmune diseases like systemic lupus erythematosus (8) or genetic conditions that can cause premature ovarian insufficiency in women, such as Turner’s syndrome or fragile X-related mental retardation, or hypogonadism and azoospermia/oligozoospermia in men, like in individuals with Klinefelter’s syndrome (reviewed in 2). Moreover, other circumstances exist in which FP must be considered, such as sex reassignment surgeries (2) or a variety of social reasons that may end up hampering or delaying parenthood to otherwise perfectly fertile couples (9). Below, currently available procedures for both women and men are addressed, as well as other procedures still at experimental stage. AVAILABLE FERTILITY PRESERVATION PROCEDURES Male FP Nowadays, two options for FP in males can be found: gonadal shielding and sperm cryopreservation. In cases in which radiotherapy is unavoidable, gonadal shielding may result helpful since it seems to mitigate the effects of radiation, especially in children (10, 11). This procedure consists in covering the testes with a lead block or apron to avoid direct exposure to radiation (10); however, it does not completely prevent from radiation damage. Therefore, the best option for FP in pubertal and adult males is most likely sperm cryopreservation (Figure 1). Even though the sample is usually collected by masturbation, it may be also obtained by other methods including testicular sperm extraction (TESE) or electroejaculation. These methods are commonly applied in cases in which the previous approach is not possible due to specific reasons, such as certain physical/psychological conditions or even religious beliefs (2, 11). Female FP Several options are currently available for FP in female patients, including oocyte and embryo cryopreservation, ovarian transposition or gonadal shielding. These options are more invasive and time-consuming than for the male counterpart, and so it is important to choose the appropriate FP procedure according to the treatment (3). Oocyte and embryo cryopreservation have been established as standard methods by the American Society of Reproductive Medicine since 2012 (3, 12) (Figure 2). Between these two techniques, oocyte cryopreservation is usually the preferred one (2); even though embryo cryopreservation is offered to women with a partner and shows great results, it may result in issues past some years; for instance, if the couple divorces or the patient does not recover from the disease (12). Both methods require medical ovarian stimulation at the beginning, as well as follicular monitoring and transvaginal oocyte retrieval. The whole process can take around two weeks (3, 11). Sometimes, harvesting of immature oocytes and the subsequent in vitro maturation may be indicated for those patients who cannot undergo controlled ovarian stimulation, like prepubertal girls or women suffering from polycystic ovarian syndrome (PCOS) (2, 13). Once the oocyte matures, it will be eventually cryopreserved (to learn more about oocyte cryopreservation, read our post on “Social egg freezing”). 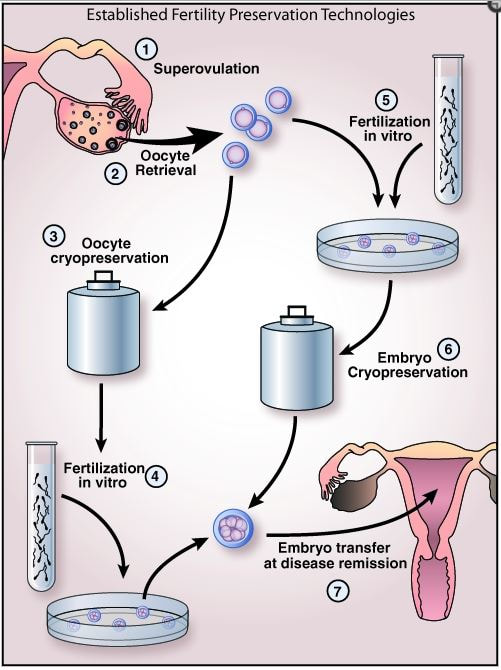 Figure 2. Oocyte and embryo cryopreservation: standard methods established for women (14). In those cases in which oocyte/embryo cryopreservation is not possible due to the urge to commence the treatment, patients may also resort to the other methods. Both gonadal shielding and ovarian transposition are indicated when radiation on the pelvic area is necessary (11, 15). Ovarian transposition requires surgical intervention to remove the ovaries and fix them, usually to the anterolateral abdominal wall. In these cases, it is recommended to collect a biopsy sample of ovarian tissue, since certain risk of failure is expected (12). EXPERIMENTAL TECHNIQUES AND FUTURE PROSPECTS The only available method for FP in prepubertal male children so far is gonadal shielding. However, the option of testicular tissue cryopreservation (TTC) is sometimes offered by some clinics, as well. This technique remains experimental and there are currently no reports on reimplantation of testicular tissue or achievement of pregnancy (11). Due to the risk of reintroducing malignant cells (2), TTC still depends on the improvement of other techniques for the maturation of spermatogonial stem cells into mature sperm, which is necessary for current assisted reproduction techniques (IVF and ICSI) (3). Regarding female FP methods, the experimental ovarian tissue cryopreservation technique is also offered by some clinics, and it is the only option for prepubertal females and for those patients who cannot delay the initiation of the treatment (3). In this technique, part of the ovarian cortex with the primordial follicles is harvested and vitrified (4). Certain studies have demonstrated successful pregnancies in patients with transplanted ovarian tissue (3) (to learn more about ovarian tissue cryopreservation, read our post “Ovarian tissue cryopreservation. Current procedures and outcomes”). Treatments with gonadotropin-releasing hormone agonists (GnRHa) are a common practise in different situations, including certain cases of infertility or sex hormone-related issues. FP approaches required in cases of chemotherapy treatments may include administration of GnRHa, since they have been proved to be efficient in keeping ovaries quiescent and reducing their regular activity. This means inhibition of the so-called hypothalamic-pituitary-gonadal axis, which is the main hormone pathway regulating ovarian and follicular activity. By administering GnRHa’s, it would be possible to reduce the blood flow to the ovary, thus preserving follicles (4), so that they can grow and mature later on once chemotherapy treatment is over. However, evidence for its efficiency is still relatively low, and so further research is still necessary on this field (4, 16). Looking into the future, potential prospectives for female FP may include in vitro activation of cryopreserved follicles within the ovarian tissue, in vitro follicle culture and development of an artificial ovary into which primordial follicles could be eventually transplanted and cultured (2). The use of stem cells has been demonstrated to have promising results in the generation of both male and female artificial gametes (2, 17). Embryonic stem cells (ESCs), induced pluripotent stem cells (iPSCs) and embryonic germ cells (EGCs) are different types of stem cells with distinct degrees of pluripotency; this means they are able to differentiate into any (or almost any) cell type and tissue present in the body (17). In human embryos, primordial germ cells (PGCs) represent the earliest stage of gametes that, after a series of reprogramming changes and differentiation, will result in sperm or oocytes in the adult. Using the above-mentioned pluripotent (or totipotent) cells, several studies have reported it possible to generate germ cells that will eventually differentiate into fully functional sperm and eggs (17). On the other hand, the use of PGCs present in the gonads of the progenitors, which are spermatogonial stem cells (SSC) in the male and ovarian stem cells (OSC) in the female, have been also studied for artificial gamete generation by in vitro propagation of SSC and by in vitro propagation and re-aggregation of OSC in the ovarian tissue (reviewed in 17). CONCLUSIONS FP is an essential issue to keep in mind in situations in which the fertility capacity is at stake, which usually happens when undergoing certain medical treatments (or other circumstances). Currently, there exist several available options for patients and people, both at prepubertal and reproductive age, who need to preserve their fertility. Even though the most used one is gamete cryopreservation, other experimental techniques, such as the ovarian/testicular tissue cryopreservation, should be born in mind. There is still a clear need for improvement of those experimental techniques, since every disease and situation are different, and because the use of gamete cryopreservation is not always a viable option. REFERENCES
1. Jeruss JS, Woodruff TK. Preservation of Fertility in Patients with Cancer. N Engl J Med. 2009;360(9):902-911. 2. Martinez F. Update on fertility preservation from the Barcelona International Society for Fertility Preservation–ESHRE–ASRM 2015 expert meeting: indications, results and future perspectives. Hum Reprod. 2017;32(9):1802-1811. 3. Burns KC, Hoefgen H, Strine A, Dasgupta R. Fertility preservation options in pediatric and adolescent patients with cancer. Cancer 2018. 4. Harada M, Osuga Y. Fertility preservation for female cancer patients. Int J Clin Oncol. 2018. 5. Vakalopoulos I, Dimou P, Anagnostou I, Zeginiadou T. Impact of cancer and cancer treatment on male fertility. Hormones (Athens). 2015;14(4):579-589. 6. Kemertzis MA, Ranjithakumaran H, Hand M, Peate M, Gillam L, McCarthy M, Super L, McQuillan S, Drew S, Jayasinghe Y, Orme L. Fertility Preservation Toolkit: A Clinician Resource to Assist Clinical Discussion and Decision Making in Pediatric and Adolescent Oncology. J Pediatr Hematol Oncol. 2018;40(3):e133-e139. 7. Joshi S, Savani BN, Chow EJ, Gilleece MH, Halter J, Jacobsohn DA, Pidala J, Quinn GP, Cahn JY, Jakubowski AA, Kamani NR, Lazarus HM, Rizzo JD, Schouten HC, Socie G, Stratton P, Sorror ML, Warwick AB, Wingard JR, Loren AW, Majhail NS. Clinical guide to fertility preservation in hematopoietic cell transplant recipients. Bone Marrow Transplant. 2014;49(4):477-484. 8. Choux C, Cavalieri M, Barberet J, Samson M, Bonnotte B, Fauque P, Sagot P. [Immunosuppressive therapy and fertility preservation: Indications and methods]. Rev Med Interne 2018. 9. Daniluk JC, Koert E. Childless women's beliefs and knowledge about oocyte freezing for social and medical reasons. Hum Reprod. 2016;31(10):2313-2320. 10. Sayan M, Cassidy RJ, Butker EE, Nanda RH, Krishnamurti L, Khan MK, Esiashvili N. Gonadal shielding technique to preserve fertility in male pediatric patients treated with total body irradiation for stem cell transplantation. Bone Marrow Transplant. 2016;51(7):997-998. 11. Saraf AJ, Nahata L. Fertility counseling and preservation: considerations for the pediatric endocrinologist. Transl Pediatr. 2017;6(4):313-322. 12. Donnez J, Dolmans MM. Fertility Preservation in Women. N Engl J Med. 2018;378(4):400-401. 13. Hirshfeld-Cytron J, Gracia C, Woodruff TK. Nonmalignant diseases and treatments associated with primary ovarian failure: an expanded role for fertility preservation. J Womens Health (Larchmt). 2011;20(10):1467-1477. 14. Shirasawa H, Terada Y. In vitro maturation of human immature oocytes for fertility preservation and research material. Reprod Med Biol. 2017;16(3):258-267. 15. Kanda Y, Wada H, Yamasaki R, Kawamura K, Ishihara Y, Sakamoto K, Ashizawa M, Sato M, Machishima T, Terasako-Saito K, Kimura S, Nakasone H, Kikuchi M, Yamazaki R, Kanda J, Kako S, Nishida J, Tsunoda H, Omori Y, Nakazawa M, Tanaka O. Protection of ovarian function by two distinct methods of ovarian shielding for young female patients who receive total body irradiation. Ann Hematol. 2014;93(2):287-292. 16. Senra JC, Roque M, Talim MCT, Reis FM, Tavares RLC. Gonadotropin-releasing hormone agonists for ovarian protection during cancer chemotherapy: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2018;51(1):77-86. 17. Vassena R, Eguizabal C, Heindryckx B, Sermon K, Simon C, van Pelt AM, Veiga A, Zambelli F; ESHRE special interest group Stem Cells. Stem cells in reproductive medicine: ready for the patient? Hum Reprod. 2015;30(9):2014-2021.
0 Comments
|
Categories
All
 2016-2019. All Rights Reserved by Embryologist Media. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License . |
Embryologist Media
