|
"Increasing efforts in making this procedure feasible and more widely available are expected, since there is a significant clinical demand" Author: Iris Martínez Rodero  CCO. Public Domain WHAT IS UTERUS TRANSPLANTATION? Uterus transplantation is a surgical technique in which a healthy and functional uterus is temporarily transplanted into a woman whose uterus is absent or dysfunctional (1, 2). Thereby, uterine transplant is a potential treatment for absolute uterine factor infertility (AUFI), where normal embryonic implantation cannot occur. AUFI causes up to 3-5% of female infertility cases worldwide, whose underlying conditions are (Figure 1) (1):
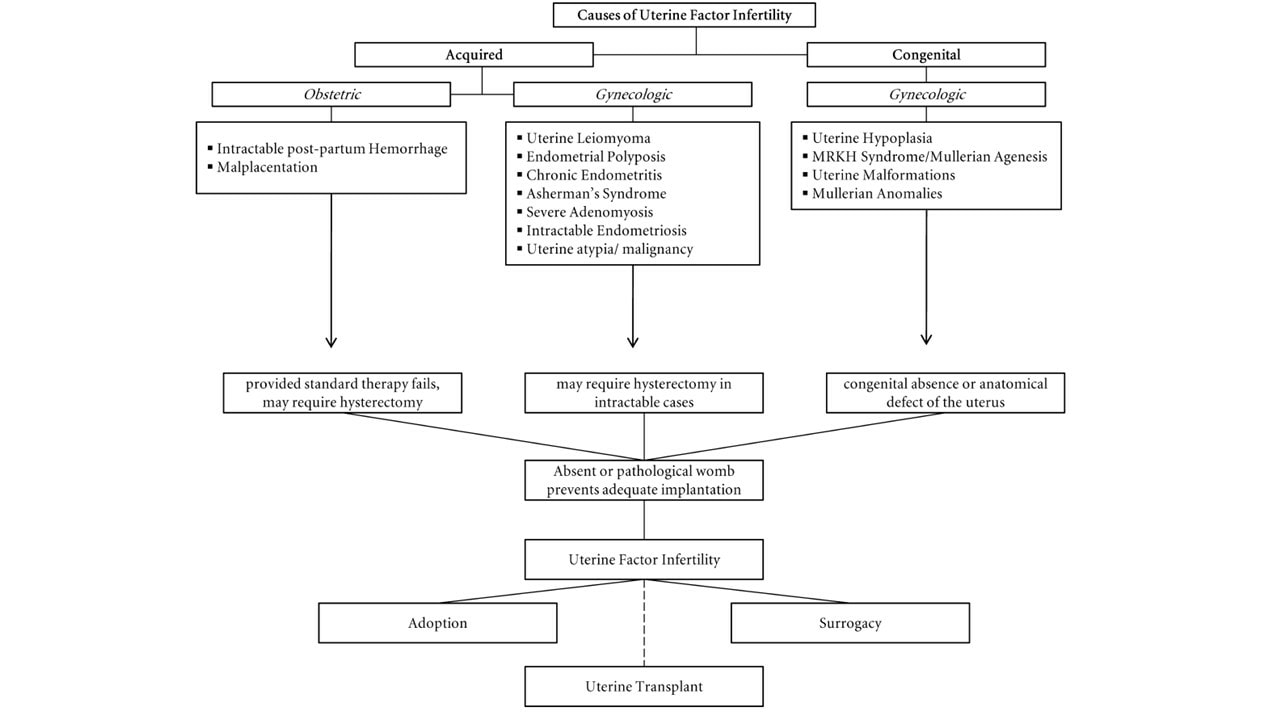 Figure 1. Causes of uterine factor infertility and the options for having offspring (1). Overview of the whole process For a uterine transplantation, both a recipient and a compatible donor are needed. The ideal approach is using a uterus from a deceased donor to avoid putting healthy women at risk (1, 2, 4). The surgery is more complicated than a standard hysterectomy (surgery where the uterus is removed), and for a living donor it entails an 11-hour long operation, with surgeons working near vital organs. It consists of the removal of the donor’s uterus, cervix, part of the vagina and other tissues necessary to attach the uterus to the recipient. It is a meticulous procedure, since tiny blood vessels need to be resected without injuring the donor. In the case of deceased donors, the organ can be removed faster since there is no risk of causing harm. Once extraction is completed, the organ can survive for at least six hours if maintained under the proper conditions (1, 4). The next step is the transplant surgery, which normally takes about five hours. In this procedure, an artery and a vein on either side of the uterus are connected to the recipient’s blood vessels, while there is no need to reconnect the nerves. Part of the donor’s vagina is stitched to the recipient’s (Figure 2). Then, the transplanted uterus is stabilized into the pelvis using supporting tissue removed from the donor (1, 4). 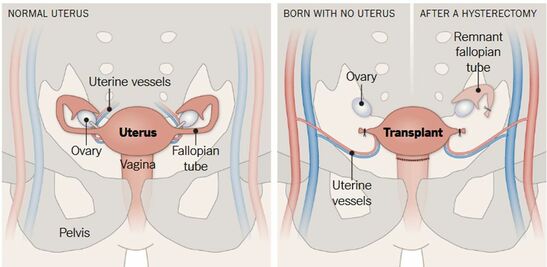 Figure 2. Uterus transplant. Surgeons remove the uterus, cervix and part of the vagina from a donor (either living or deceased). Small uterine vessels are also preserved so they can carry blood to the organ. The uterus is then stitched to the recipient’s vagina and the small uterine vessels are connected to large blood vessels. If present, the recipient’s ovaries are moved away and remnant Fallopian tubes are not in contact with the transplanted uterus. One year after the surgery, the recipient may undergo embryo transfer procedures (4). Given that the recipient Fallopian tubes are not be connected to the transplanted uterus, a natural pregnancy will be impossible. Therefore, the embryo is conceived by in vitro fertilization, which can be performed either before or, preferably, after transplantation (1, 4). For a full recovery from surgery to be achieved and in order to adjust the right doses of immunosuppressant/anti-rejection medicine, normally a whole year is required (Figure 3). Past this time, the patient can try to conceive. As previously mentioned, the doctors will transfer one in vitro fertilized embryo at a time into the uterus, until pregnancy is achieved. Subsequently, in order to avoid the transplanted uterus undergoing the stress of delivering the baby, a caesarean section is performed before the due date (1, 4). After delivery the uterus can be kept, should the mother want to try to conceive again eventually. For safety reasons, the limit is set for two babies per transplanted uterus. In case the woman does not wish to conceive another child she may decide to have the uterus removed through hysterectomy, so she can stop taking the immunosuppressant medication (1).  Figure 3. Uterine transplantation timeline (1) Complications of uterine transplantation Transplantation is a hugely complex intervention; not only does it involve potential complications of surgery as postoperative bleeding, possible infections or atrial fibrillation, but also immune rejection of the transplanted organ. To avoid an immune reaction, immunosuppressants need to be taken after transplantation. Since these weaken the immune system, infections and tissue recovery are even more complex to solve (1, 2, 4, 5). CHRONOLOGY OF UTERINE TRANSPLANTATION: FROM TRIALS ON ANIMALS TO CURRENT SUCCESSFUL ATTEMPTS In the early 50’s, the first trials of uterus transplantation were performed in various animal models, including primates (1, 2). What is considered to be the world’s first clinical uterus transplantation is a trial performed by Fagee and his team in Saudi Arabia in 2000. The surgery was proved technically possible, even though the uterus was removed 100 days later due to a necrosis episode (5). Nonetheless, more trials were carried out along the years, mainly in Turkey, where uteri from deceased donors or attained pregnancies were used, all of them ending in miscarriages (1). In 2014, the first delivery of a healthy baby from a donor uterus was achieved. This event, led by Mats Brännström from Gothenburg University in Sweden, opened the doors to the feasibility of uterus transplantation and prompted new areas of clinical and basic research (6). Nowadays, at least 12 healthy babies have been born from uterine transplantation (1). Until 2017, all babies had been born from uteri donated by living women. Several attempts of uterus transplantation from deceased donors had been surgically successful, but the first healthy baby was born on Dec 15, 2017 in Hospital das Clínicas, University of São Paulo, Brazil (7). A summary of both successful and unsuccessful uterus transplantation attempts reported in the literature is shown below (Table 1): 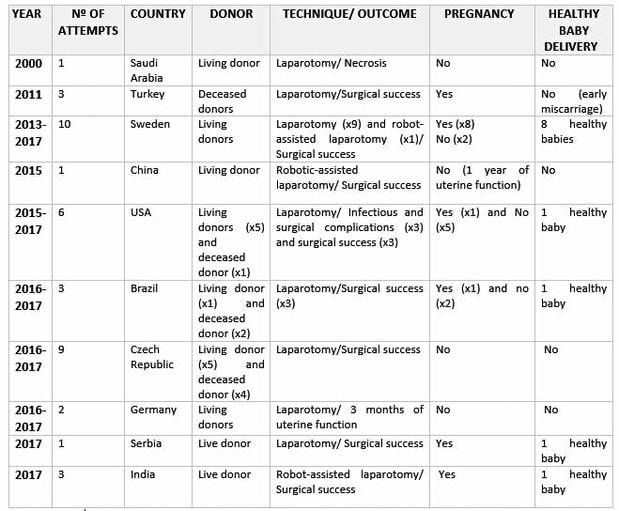 Table 1. Uterine transplantation clinical trials from 2000 to 2018 (1,6,7,8) RISK-BENEFIT ANALYSIS Currently, women suffering from uterine infertility who wish to have offspring carrying their genetic background can turn to surrogacy combined with in vitro fertilization techniques to accomplish their desire. By “borrowing” or “renting” the womb of another woman, a baby conceived in vitro from the gametes of the infertile couple can be born (2). However, surrogacy not only does give rise to multiple ethical controversies, but it is also outlawed in many countries, such as Spain or Italy. Surrogacy is perceived as damaging the dignity of motherhood, while turning babies into a commodity, often resulting in negotiations and litigations. In this sense, some authors position uterus transplantation as a “more ethical” alternative to surrogacy (2, 4, 5). Aside from ethical concerns, uterine transplantation is often considered to be more feasible because it allows the recipient to experience gestation and labour, whereas surrogacy does not (2). It is worth noting that 97.5% of women who underwent a survey in the UK, where surrogacy is legal, preferred uterine transplantation over gestational surrogacy or adoption (9). Furthermore, a recent survey in Japan revealed that uterine transplant was two times more accepted than gestational surrogacy among among 3,892 women from the general population aged 25 to 39 (10). In Sweden, 2000 out of 3500 randomly selected women aged 30-39 preferred uterine transplant over surrogacy (11). Nevertheless, uterus transplant is still a very complex surgical procedure, which presents significant health threats and does not guarantee a successful, healthy pregnancy. Medical staff should therefore inform patients about the risks inherent to the procedure, particularly about the hazards of immunosuppressant treatment typical of a transplant. In this case, immunosuppressant drugs may nullify the purpose of the transplant itself, as they can result in injury to the foetus and even lead to its death (1, 2, 5). Moreover, women should be warned that, as there is no nerves reconnection, they will not perceive the fetus pressing against the inner walls neither will they feel the transplanted womb contractions (2). All the above mentioned, it is clear that a risk-benefit ratio of uterus transplantation should be carefully assessed and described in each case. ETHICAL REMARKS UterIne transplantation entails multiple medical, ethical and legal issues, involving both donors and recipients. That is why in 2012, Lefkowitz and colleagues from McGill University in Canada proposed “the Montreal Criteria” (Figure 4). This is a set of proposed criteria required for a woman to be considered a candidate for uterine transplant, and ethically and medically approved (2, 3). 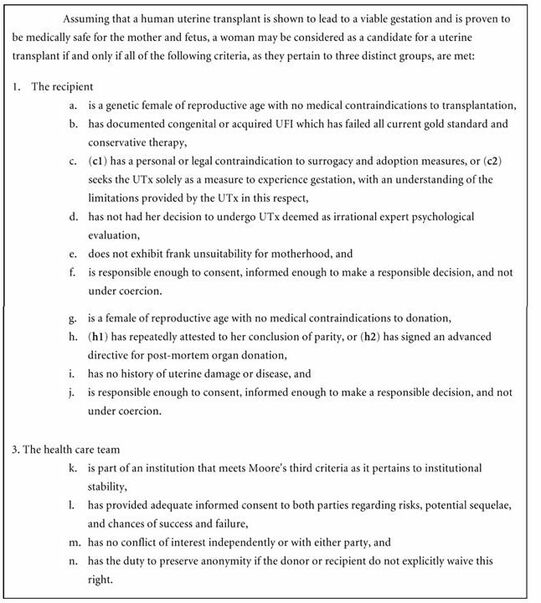 Figure 4. The Montreal Criteria (3).
CONSEQUENCES FOR DONORS, RECIPIENTS AND CHILDREN Possible implications for donors, recipients and children have not been yet studied. If uterus transplantation becomes a routine procedure, a multi-disciplinary team effort would be necessary to monitor uterus donors, recipients and babies (1). There exist a few results about long-term psychological strains in living donors (1, 12). In a observational study conducted by Brännström et al. in the 1-year follow up, the donors were asked if they had returned to predonation mental health, if they had any regrets and if they had returned to previous activities both professionally and privately (12). They concluded all donors returned to their predonation levels of physical health (12). Other 'side effects' were similar or comparable to minor medical and surgical complications, which were actually reversible and could be solved shortly after the surgery. Still, the absence of long-term complications should be confirmed (1, 5). Regarding recipients, an established program of follow-up should be defined, which would consist of medical exams and psychological assessments (1). Additionally, the study should continue to monitor the wellbeing of the recipients even after they have delivered their babies and had the uterus removed (1, 2). The surgery for the transplanted uterus removal would be planned after the delivery of the desired number of babies (1, 2, 5). To date, all children born after uterus transplantation have been reported to be healthy. However, they developed inside a womb that might have been taken from a deceased donor, and so it could have been exposed to anti-rejection drugs (5,6). Since possible side-effects might be detected at a later stage, a registry should be created in order to collect all possible information about their long-term health (1, 5). FUTURE PROSPECTS FOR UTERUS TRANSPLANT Tissue engineering and the creation of artificial organs is a promising field that would dramatically improve the current situation of transplants (13). Uterus transplant would benefit from that kind of advances, as second-party donors and immunosuppressive therapy would not be needed. Although a human bioartificial uterus is far from being ready for clinical application, there are some promising results in animals (14, 15, 16). CONCLUSIONS Women who suffer from uterine factor infertility need to rely on surrogacy to fulfill their wish to conceive their own offspring. Nevertheless, surrogacy is illegal in many countries, whereas uterus transplantation can be a sustainable and ethically acceptable alternative for patients who wish to achieve motherhood. From an experimental point of view, uterus transplantation has evolved rapidly from its origin in animal models to its current successful clinical application. However, this should still be regarded as an experimental procedure, and a risk-benefit analysis is due on a case-by-case basis to ensure it is applied in an ethical and appropriate manner. A detailed registry of surgical outcome and reported complications and side effects needs to be collected from clinical trials before uterus transplant becomes a routine procedure. Increasing efforts in making this procedure feasible and more widely available are expected, since there is a significant clinical demand. REFERENCES
0 Comments
Leave a Reply. |
Categories
All
 2016-2019. All Rights Reserved by Embryologist Media. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License . |
Embryologist Media
