|
Authors: Shuyana Deba, Javier Del Río, Isabel Sánchez and Sara Sanz 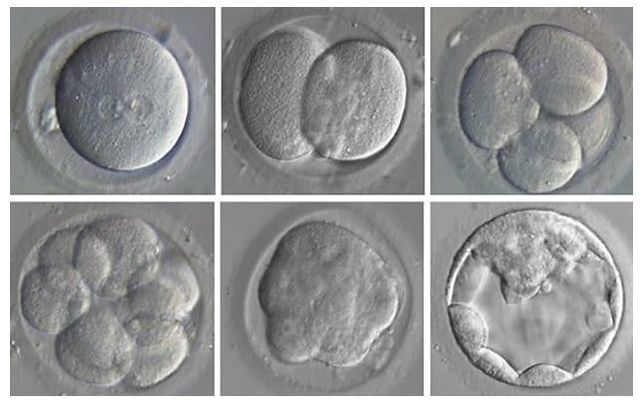 Figure 1. Embryonic development (1) Fertilization is a sequence of coordinated events that results in the metabolic activation of the ootid (nearly mature oocyte) and triggers cleavage of the zygote (2). Nowadays, in assisted reproduction laboratories cleavage can be evaluated in vitro and in real time. Once in vitro fertilization (IVF) has been accomplished, early development of the embryo can be recorded by using time-lapse systems (TLP) (3). This approach makes it possible to evaluate morphology, including dynamic parameters, based on the uninterrupted culture of the embryo, which also allows for a better embryo selection, thus rising pregnancy rates (4). Even so, there are still clinics all over the world that select embryos for transfer using light microscopy, which means the use of a conventional incubation method (5). CRITERIA FOLLOWED FOR EMBRYO CLASSIFICATION It is known that an international consensus is needed in the way embryos are assessed and described. The following standardized criteria is from Alpha Scientists in Reproductive Medicine and ESHRE Special Interest Group of Embryology, 2011 and includes ‘minimum standards’ for oocyte and embryo morphology scoring (6): the current expected observation for embryo development is 4 cells on day 2 and 8 cells on day 3 after fertilization (day 0). Moreover, embryos with <10% fragmentation, stage-specific cell size and not multinucleated are considered of good quality (6). According to this consensus, scoring for day 4 (morula stage) regards as good embryos those that enter into a fourth round of cleavage, which implies evidences of compaction that virtually involve the whole volume of the embryo (6). Finally, on day 5 blastocysts are to be observed expanded with: a prominent inner cell mass (ICM) consisting of many cells, compacted and tightly adhered together; and a trophectoderm (TE), forming a cohesive epithelium (6). Nevertheless, these parameters do not restrict laboratories to annotate further observations in order to select the best embryo for transfer (6). BEST DAY TO PERFORM EMBRYO TRANSFER One of the most important aspects that influence the success of ART is embryo transfer from the culture medium to the uterus (7). This has been a controversial subject that still generates quite some doubts. Morphological evaluation of embryos is sometimes a subjective process, and it provides limited information on the possible genetic abnormalities that embryos may have (8). Currently, there exists a great controversy on the optimal moment to carry out embryo transfer.
IN WHICH CASE DOES THIS TRANSFER USUALLY TAKE PLACE? Day 2 transfer is usually indicated in cases of poorly responding patients. Indeed, it is also indicated when the sperm, oocyte and/or embryos are also of low quality and/or number (9, 10, 11). WHAT DO EXPERTS SAY? Several retrospective studies have compared embryo transfer on day 2, day 3 and day 5 after oocyte recovery, all of which presented conflicting results. A study performed by Mahdavi et al. among poor responder patients revealed no clinical differences between day-2 and -3 embryo transfer (10). However, this study found that pregnancy rates per oocyte retrieval and embryo transfer were significantly higher in the day-2 embryo transfer group compared to day 3 group. It is worth mentioning that other investigators did not find significant differences in pregnancy outcomes when they compared embryo transfer on day 2 and day 3 (11, 12). Additional results from other studies have revealed higher clinical and ongoing pregnancy rates after embryo transfer on day 2 than on day 3 in poor responders. This suggests that the occurrence of miscarriage can be reduced by restricting embryo culture to only 2 days, which could also provide an alternative for managing poorly responding patients (11). That is the reason why embryo transfer on day 2 is still performed in many IVF centres; there is an actual risk of compromising the viability of embryos by prolonged in vitro culture in sub-optimal conditions, with an increased risk of obtaining no blastocysts to replace on day 5 (9, 13, 14). Even though there seems to be a large number of benefits for these patients, certain disadvantages that may potentially occur must also be taken into account, as it can be seen below (Table 1). 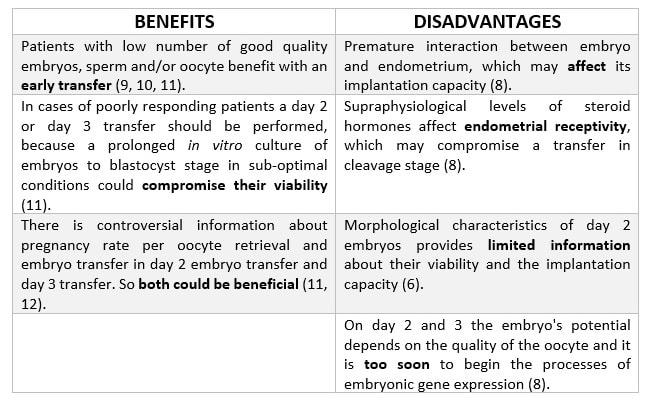 Table 1. Benefits and disadvantages of transferring D+2
PATIENTS IN WHICH TRANSFER D+3 SHOULD BE PERFORMED There exists no criterion to select patients who should be transferred on D+3. Traditionally, embryo transfer has been performed on cleavage stage, so the chosen day was D+3 of embryo development (7). Generally speaking, embryo transfer was carried out on this day in all patients, until a culture medium was developed that allowed to keep embryos in the laboratory for 5-6 days, and with the exception of the cases previously mentioned (11). SCIENTIFIC LITERATURE TO SUPPORT D+3 AS THE BEST DAY FOR EMBRYO TRANSFER Many studies show contradictory results on whether it is better to transfer on D+2 or D+3. However, there are no significant differences as for implantation, clinical pregnancy or live birth rates when comparing transfer on these days. A study by Modares et al. (15) with patients under 40 years old showed a slight improvement in these results when transferring on D+3, although differences were not significant. The authors also showed embryo quality to be worse when the transfer was performed on D+3 than on D+2. Thus, implantation rate has been observed to be higher in D+3, because extending embryo culture for one day allows to discard those embryos that stop their development from D+2 to D+3 (16, 17). Furthermore, it is necessary to consider that there are other external factors that affect embryo development and, consequently, the selection of the best day to transfer. Quinn et al. (18) determined that one of these factors is culture media. Thus, in sub-optimal lab conditions, it would be interesting to transfer on D+2 rather than D+3, in order to spend the shorter time possible in the media. Regarding D+5 transfer, some studies have shown higher implantation rates in embryos transferred on the blastocyst stage compared to those transferred on D+3 (cleavage stage). However, it is necessary to consider that only 25% of embryos reach the blastocyst stage (15); this implies that the number of embryos transferred and vitrified in a cycle is lower than for D+2 and D+3. As a consequence, when considering cumulative pregnancy rates no significant differences are found between transferring on cleavage stage and blastocyst (7). Again, benefits for the patients must be considered along with potential disadvantages (Table 2). 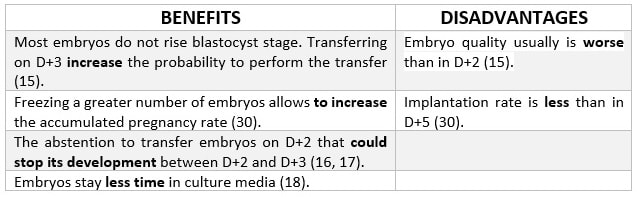 Table 2. Benefits and disadvantages of transferring D+3
It has been observed that transfer on blastocyst stage helps to improve pregnancy rates and reduce the risk of a multiple pregnancy. Why? One reason might be that there is no method to determine whether embryos that initially seem to be of good quality are likely to develop up to blastocyst (19). WHO ARE THE IDEAL PATIENTS? 1. Those with a large number of embryos (20). 2. Those whose day-3 embryos are of good quality (20). 3. Those in which day-1 embryos exhibit pro-nuclei and present a grading profile (20). 4. Young women with good ovarian response (21). 5. Those whose embryos display an early cleavage (22). POTENTIAL BENEFITS OF BLASTOCYST-STAGE TRANSFER vs. CLEAVAGE-STAGE TRANSFER First of all, the new culture media allow us to perform longer incubations in the laboratory, after which the best embryos can be selected with higher accuracy and with lower risk of aneuploidies (23). Moreover, there will exist a better synchronization between the embryo and the mother. Additionally, uterine contractility decreases during the luteal phase (24, 25). The size of these blastocysts is bigger, so some studies have found fewer cases of ectopic pregnancies in comparison to transfers on day 3 (26). A parallel comparison of benefits vs. disadvantages for this procedure can be seen in below (Table 3). 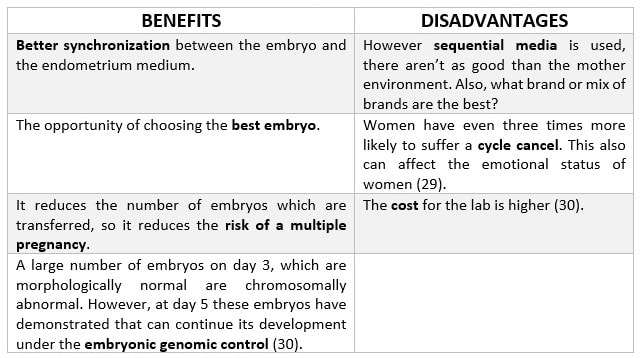 Table 3. Benefits and disadvantages of transferring blastocysts (27) IS IT BETTER TO TRANSFER ON DAY 5 OR ON DAY 6?
The optimal time for embryo transfer depends on a variety of factors, such as the embryo growth speed. However some studies have revealed both implantation and pregnancy rates to be more successful when embryos are transferred on day 5 compared to day 6. This is due to the fact that viability of embryos expanded on day 5 is higher than for those expanded on day 6 (30). In conclusion, it seems difficult to define the most appropriate day for embryo transfer to be applied for each patient. Therefore, every single case must be individually analyzed. In addition, several factors should be taken into account when deciding on the day for embryo transfer, such as maternal age, sperm and oocyte quality or physiological response of the woman and/or the available embryos. By doing so, a good decision can always be made in order to improve implantation and pregnancy rates. REFERENCES
13 Comments
|
Entries
March 2019
Categories
All
 2016-2019. All Rights Reserved by Embryologist Media. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License . |
Embryologist Media
