|
Authors: Belén Gómez Giménez and Edel Rocher "The assessment of embryo development in vitro suggests that collapsing of the blastocoel might be indeed related to a certain degree of success"  Figure 1. Artificial shrinkage of blastocoelic cavity in human expanded blastocysts by hyperosmotic sucrose solutions, before and after the treatment (1). One of the main factors related to embryo selection for transfer is the extension of embryo culture up to blastocyst stage. This approach has been demonstrated to improve clinical outcomes after in vitro fertilization IVF (2). Consequently, in the last couple decades a specific blastocyst grading system has been applied to assess embryo morphology during blastocyst stage (appearance of the inner cell mass (ICM) and the trophectoderm (TE)) [read our post on blastocyst assessment]. But there are other aspects about blastocyst development to focus on, such as the study of collapse and re-expansion in vitro and how it could affect implantation and pregnancy rates. BLASTOCYST COLLAPSE UNDER NORMAL CIRCUMSTANCES The term "collapse" refers to the contractions observed in the blastocyst that respond to a series of physical phenomena related to its proper development. Once morula stage has been reached, the forming blastomeres begin to pump ions through the Na+/K+ machinery (3). This entails an implicit osmotic response that results in the accumulation of water in the cavity thus formed, the blastocoel. The progressive accumulation of water causes the blastocyst to grow in size from early stages, consequently increasing the hydrostatic pressure between the TE and the zona pellucida (ZP) until the blastocyst hatches (4, 5). The efflux of the blastocoel fluid through loose cell bindings in the already formed TE causes the aforementioned contractions or "collapse". This phenomenon was originally called "blastocyst breathing", due to the sequence of collapse and re-expansion events observed in the rupture of the ZP during blastocyst hatching (6). However, the mechanisms of blastocoel collapse and TE recovery after the rupture in vitro still remain unclear (7). INFLUENCE OF THE NATURAL COLLAPSE OF BLASTOCYSTS ON REPRODUCTIVE OUTCOMES When considering the effect of blastocyst collapse on future outcomes, certain aspects must be taken into account: 1. Number of collapsing episodes Nowadays, there are still few studies on the frequency of blastocyst collapse. Marcos and coauthors (2015) focused on this aspect for the first time and reported almost a 20% of single collapse episodes in a total of 715 blastocysts, whereas only about 1.5% exhibited multiple collapse events (8). Independent authors have further studied this topic; even though they all have shown significant variations in the percentages of both single and multiple collapse events during blastocyst stage (8, 9), results do suggest a correlation between the number of collapsing episodes and the future outcome for the blastocyst (7, 8, 9). 2. Effect of collapse on blastocyst hatching Research on certain mammalian species had shown that blastocysts with smaller contractions (collapse/re-expansion events) were more likely to reach the hatching stage than those with large strong contractions (10, 11, 12). Results in patients showed that differences in hatching rates were not statistically significant between blastocysts with and without collapse (28.7% vs 31%, respectively) (7). However, hatched embryos with previous collapse episodes exhibited lower implantation rates than those with no collapse (35.1% vs 48.5%, respectively) (8). Taken together, these results indicate the process of collapse and re-expansion may not have a direct influence on blastocyst development up to the hatching stage, but they seem to negatively affect the success rate of such blastocysts after implantation in the uterus. 3. Relationship between standard morphological evaluations and blastocyst collapse Morphological assessment of embryos has also been used in order to figure out the main cause for blastocyst collapse. This evaluation has been performed considering the number of blastomeres, level of fragmentation and quality in days 2, 3 and 5 (blastocyst stage). Nevertheless, the comparison between all these standard morphological features did not yield significant differences that could relate to the event of blastocyst collapse (6, 8). Whereas further evaluation is a usual practice for non-hatched blastocysts, these studies showed no results regarding day 6. Although comparisons including this factor may potentially reveal connections between collapsing of blastocysts and their early developmental history, no data are currently available on this issue. 4. Prediction value of morphokinetic variables The evaluation of morphokinetic variables has proven to be useful in selecting embryos for transfer, given their potential to predict the successful development of the embryo. These variables have been associated with blastocyst formation, implantation potential and aneuploidy status (13, 14, 15), measured in different critical steps of embryo development (16). In spite of the increasing amount of studies focused on the relation between morphokinetic values and embryo implantation rates, only a few studies can be found that link these variables with the occurrence of blastocyst collapse (7, 9). Marco et al (2015) showed a significantly slower development of those embryos that had not collapsed, compared to those that did, considering development times from 2-cell stage up to blastulation (t2 - tB, respectively) (7). These results are found difficult to combine with those by Bodri and colleagues (2016); although the authors did relate blastocyst collapse to a progressively decreased live birth rate, they were not able to state this feature as a valid predictor of embryo survival on its own (9). ARTIFICIAL SHRINKAGE As it has been previously discussed, blastocyst collapse is a natural phenomenon linked to normal blastocyst development. Even though previous data have shown no direct correlation between this feature in vivo and implantation rates, recent and current studies in vitro suggest that the occurrence of blastocyst collapse has indeed a significant effect on the clinical outcome of the embryo, as explained below. Currently, vitrification is a widely spread practice in laboratories, aimed to preserve cells/tissues/organs at ultralow temperatures (-196°C). It is well known that the traditional slow freezing approach for cryopreservation frequently leads to ice crystal formation that may damage the cell/tissue, thus decreasing its quality. This associated issue has been avoided by the addition of high concentrations of cryoprotectants and a significant rise in the speed of temperature drop. Such a combination increases the viscosity of the solution and turns it into a glass-like structure (17). Supporting evidence of the success of this technique are numerous studies that demonstrate that the quality of vitrified embryos is comparable to the quality of fresh ones [find more about the success of frozen blastocysts on our previous post here]. A number of researchers have concluded that blastocoel size at the moment of vitrification has an effect on embryo survival and implantation rates. The authors postulated that a large fluid-filled cavity in expanded blastocysts may inhibit sufficient permeation of the cryoprotectant into the blastocoel, thus allowing ice formation and decreasing the chances of survival (18, 19). There exist several ways to reduce the size of the blastocoel in expanded blastocysts (D5-D6) through artificial shrinkage (AS). Some of them are summarised below:
In 2002, Vanderzwalmen and collaborators achieved AS by introducing a needle into the blastocoel until blastocyst contraction was observed (18). However, and even though the authors reported an increase in survival and implantation rates compared to intact blastocysts, the increase in pregnancy rates was not statistically significant. Similar results were achieved by Son et al (2003), who induced AS prior vitrification, obtaining about 90% of blastocyst survival. Having implanted almost a third of the total, 48% of those turned into a clinical pregnancy (21). However, these studies were regarded as invasive, due to the injury the method caused in the ZP and the TE. In 2004, Hiraoka et al reported AS of the blastocoel by mechanical pipetting using a fine hand-drawn glass pipette. Even though this method also harms the TE, consequences are less severe due to the needles used. These authors also observed increased survival and pregnancy rates after AS (22). 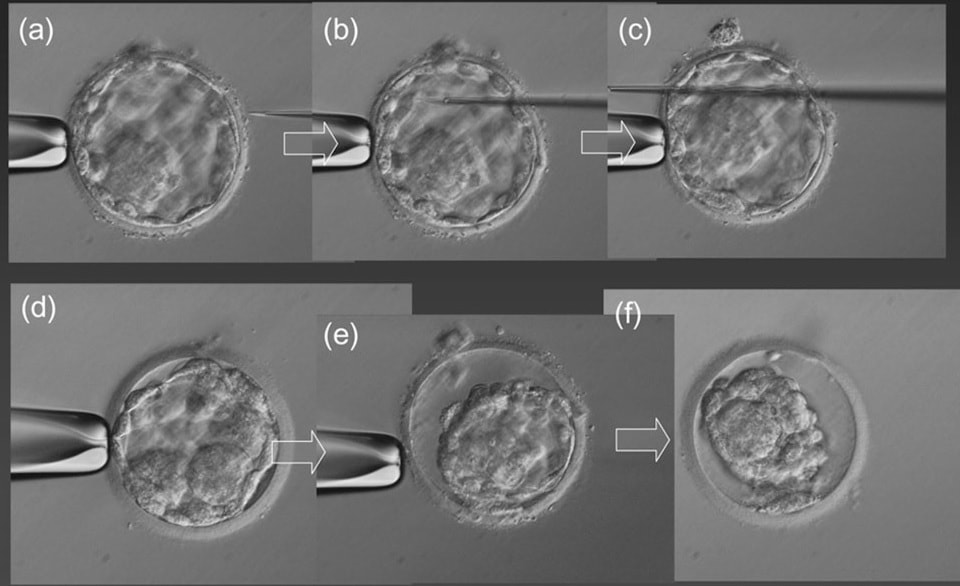 Figure 2. Artificial shrinkage (AS) of expanded blastocyst with the micro-needle: (a) holding the expanded blastocyst with the holding micropipette. (b) Insertion of the micro-needle inside the blastocoel at a point away from the ICM. (c) Puncture through the blastocoel and gradual removal of the micro-needle. (d) Beginning of shrinkage 10 s after puncture. (e) Partial shrinkage 30 s after puncture. (f) Complete shrinkage 1 min after puncture. Magnification is ×400 (23). Laser pulse has been also previously used for AS. Application of this method has reported survival rates to reach 97% and pregnancy rates up to 60% (23). In a randomized study, Van Landuyt et al (2015) found no significant increase in implantation rates after applying the pulse prior vitrification, but they did report higher post-warming blastocyst survival rate and quality in collapsed blastocysts (19). After AS, blastocysts were more likely to reach the hatching stage than those not subjected to the procedure. Similar results were obtained by Darwish et al (2016), who observed improved blastocyst survival, clinical pregnancy and implantation rates after removal of the blastocoel fluid (24). In addition, artificially collapsed blastocysts before vitrification have been recently found to re-expand more rapidly after warming (25). However, differences in live birth rates were not significant and the sample size used in the study may have been too small, so these results should be taken carefully. Other methods have been employed for AS, too. In fact, compared studies have been performed to assess differences on the protocols that may result in improved clinical outcomes. Laser pulses applied on cell-to-cell junctions on the TE and exposure of blastocysts to hyperosmotic sucrose solutions both provided evidence of increased probability of fast-developing embryos and higher implantation rates (1). Even though the authors found no significant differences between methods, the latter was suggested based on the cost/benefit ratio. These and similar results suggest that AS of human expanded and hatching blastocysts is actually a useful approach to improve clinical outcomes, regardless of the methodology employed. However, and even though it seems that collapse of the blastocoel might be indeed somehow linked to higher implantation and/or pregnancy rates, conclusions should be still drawn carefully. CONCLUSIONS Blastocyst collapse has been found to be an inherent trait of embryo early development. Its occurrence seems to be related to the physical normal progression of the embryo, and depending on the normal microenvironmental conditions, starting at the zygote stage and expanding up to the last moments before hatching and implantation. Whereas there is no compelling evidence of a link between blastocyst collapse and implantation success in natural pregnancies, the assessment of embryo development in vitro suggests that collapsing of the blastocoel might be indeed related to a certain degree of success. Comparisons between different AS methods have revealed different behaviour of blastocysts after implantation, and even an increasing number of collapsing episodes may be related to a decreased implantation potential. It is also worth to be noted the importance of vitrification in the routine practice in the laboratory; even though this process optimizes cryopreservation of cells and tissues, the integrity of the embryo may result compromised. Should this be true, blastocoel collapse may become more evident after warming of the embryos, or simply these blastocysts are more prone to collapsing, thus existing correlation rather than causation between both events. Because blastocyst collapse has been payed attention to in laboratories for just a few years now, thorough and more insightful studies are required to clarify a real connection between this feature and the outcomes of clinical pregnancies. REFERENCES
(1) Iwayama H, Hochi S, Yamashita M. In vitro and in vivo viability of human blastocysts collapsed by laser pulse or osmotic shock prior to vitrification. J Assist Reprod Genet. 2011;28(4):355-61. (2) Blake D, Farquhar CN, Johnson N, Proctor M. Cleavage stage versus blastocyst stage embryo transfer in assisted conception. Cochrane Database Syst Rev 2007; 4: CD002118. (3) Baltz JM, Smith SS, Biggers JD, Lechene C. Intracellular ion concentrations and their maintenance by Na+/K(+)-ATPase in preimplantation mouse embryos. Zygote 1997; 5: 1–9. (4) Biggers JD. Reflections on the culture of the preimplantation embryo. Int J Dev Biol 1998; 42: 879–884. (5) Watson AJ, Natale DR, Barcroft LC. Molecular regulation of blastocyst formation. Anim Reprod Sci 2004; 82–83: 583–592. (6) . Veeck LL, Zaninovic N. Human blastocysts in vitro. In: Veeck L, Zaninovic N (eds). An Atlas of Human Blastocysts. Parthenon Publishing 2003; 99–137. (7) Marcos J, Pérez-Albalá S, Mifsud A, Molla M, Landeras J, Meseguer M. Collapse of blastocysts is strongly related to lower implantation success: a time-lapse study. Human Reproduction 2015; 30 (11); 2501–2508. (8) Esbert M, Marconetto A, Soares SR, Quera M, Molina J, Florensa M, Ballesteros A, Meseguer M. Does the blastocyst collapse respond to a biological need? The analysis of 1,952 embryos by time-lapse can give an answer. Fertil Steril 2017; 108 (3, Supplement):e157. (9) Bodri D, Sugimoto T, Yao Serna J, Kawachiya S, Kato R, Matsumoto T. Blastocyst collapse is not an independent predictor of reduced live birth: a time-lapse study. Fertil Steril. 2016; 105(6): 1476-1483. (10) Erbach GT, Biggers JD, Manning PC, Nowak RA. Localization of parathyroid hormone-related protein in the preimplantation mouse embryo is associated with events of blastocyst hatching. J Assist Reprod Genet 2013; 30: 1009–1015. (11) Gonzales DS, Jones JM, Pinyopummintr T, Carnevale EM, Ginther OJ, Shapiro SS, Bavister BD. Trophectoderm projections: potential means for locomotion, attachment and implantation of bovine, equine, and human blastocysts. Hum Reprod 1996; 11: 2739–2745. (12) Seshagiri PB, Sen Roy S, Sireesha G, Rao RP. Cellular and molecular regulation of mammalian blastocyst hatching. J Reprod Immun 2009; 83: 79–84. (13) Cruz M, Garrido N, Herrero J, Perez-Cano I, Munoz M, Meseguer M. Timing of cell division in human cleavage-stage embryos is linked with blastocyst formation and quality. Reprod Biomed Online 2012; 25: 371–381. (14) Dal Canto M, Coticchio G, Mignini Renzini M, de Ponti E, Novara PV, Brambillasca F et al. Cleavage kinetics analysis of human embryos predicts development to blastocyst and implantation. Reprod Biomed Online 2012; 25: 474–480. (15) Campbell A, Fishel S, Bowman N, Duffy S, Sedler M, Hickman CF. Modelling a risk classification of aneuploidy in human embryos using non-invasive morphokinetics. Reprod Biomed Online 2013; 26: 477–485. (16) Meseguer M, Herrero J, Tejera A, Hilligsoe KM, Ramsing NB, Remohi J. The use of morphokinetics as a predictor of embryo implantation. Hum Reprod 2011; 26: 2658–2671. (17) Armitage WJ. Cryopreservation of animal cells. Symp Soc Exp Biol. 1987;41:379-93. (18) Vanderzwalmen P, Bertin G, Debauche C, Standaert V, van Roosendaal E, Vandervorst M et al. Births after vitrification at morula and blastocyst stages: effect of artificial reduction of the blastocoelic cavity before vitrification. Hum Reprod. 2002;17(3):744-51. (19) Van Landuyt L, Polyzos NP, De Munck N, Blockeel C, Van de Velde H, Verheyen G. A prospective randomized controlled trial investigating the effect of artificial shrinkage (collapse) on the implantation potential of vitrified blastocysts. Hum Reprod. 2015;30(11):2509-18. (20) Bedient CE, Khanna P, Desai N. Laser Pulse Application in IVF. In: InTech. Lasers - Applications in Science and Industry. Las Vegas. 2011. p. 204. (21) Son WY, Yoon SH, Yoon HJ, Lee SM, Lim JH. Pregnancy outcome following transfer of human blastocysts vitrified on electron microscopy grids after induced collapse of the blastocoele. Hum Reprod. 2003;18(1):137-9. (22) Hiraoka K, Kinutani M, Kinutani K. Blastocoele collapse by micropipetting prior to vitrification gives excellent survival and pregnancy outcomes for human day 5 and 6 expanded blastocysts. Hum Reprod. 2004;19(12):2884-8. (23) Mukaida T, Oka C, Goto T, Takahashi K. Artificial shrinkage of blastocoeles using either a micro-needle or a laser pulse prior to the cooling steps of vitrification improves survival rate and pregnancy outcome of vitrified human blastocysts. Hum Reprod. 2006;21(12):3246-52. (24) Darwish E, Magdi Y. Artificial shrinkage of blastocoel using a laser pulse prior to vitrification improves clinical outcome. J Assist Reprod Genet. 2016;33(4):467-71. (25) Kovačič B, Taborin M, Vlaisavljević V. Artificial blastocoel collapse of human blastocysts before vitrification and its effect on re-expansion after warming - a prospective observational study using time-lapse microscopy. Reprod Biomed Online. 2018;36(2):121-9.
0 Comments
|
Entries
March 2019
Categories
All
 2016-2019. All Rights Reserved by Embryologist Media. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License . |
Embryologist Media
