|
"The underlying cause for endometriosis is likely to present a multifactorial origin" Authors: Javier del Río, Noemi Díaz & Edel Rocher 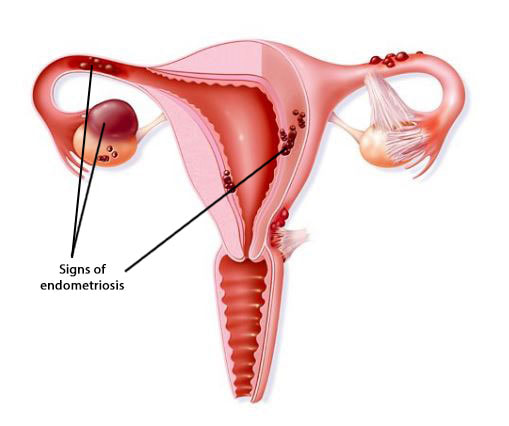 Figure 1. Illustration showing evidences of endometriosis found in specific locations of the female reproductive organs [1]. Endometriosis is defined as the presence of endometrial tissue outside the uterus, which induces a chronic inflammatory reaction. It is generally assumed that lesions arise through retrograde endometrial tissue loss during menstruation, coelomic metaplasia and lymphatic spread in immunologically and genetically susceptible individuals. Associated symptoms usually have an impact on the general physical, mental and social well-being (2,3,4). This condition is found in women from all ethnic and social groups, predominantly in those of reproductive age, which may represent an estimation of up to 176 million women all over the world. The prevalence of endometriotic disease seems to be around 5%, normally reaching a peak somewhere between ages 25 and 35. Among women aged 15-49, an annual incidence of endometriosis of 0.1% has been reported (2,3,4). Which symptoms may be indicative of the disease? Women who suffer from endometriosis typically experiment abdominal pain and related symptoms such as dysmenorrhoea, dyspareunia, heavy menstrual bleeding, non-menstrual pelvic pain, painful ovulation, dyschezia and dysuria, as well as chronic fatigue. Endometriotic lesions are followed by denervation and reinnervation, which represent accompanying changes in the central nervous system (central sensitization), thus generating a chronic pain syndrome. The extent of the disease varies from a few, small lesions on otherwise normal pelvic organs to large, ovarian endometriotic cysts (endometriomas) and/or extensive fibrosis and adhesion formation, causing marked distortion of the pelvic anatomy (2,3). As a consequence, establishing the diagnosis of endometriosis on the basis of symptoms alone may result difficult, not only due to their high degree of variation, but also because there is so much overlapping with other conditions such as irritable bowel syndrome or pelvic inflammatory disease. Therefore, it is common to come across a delay of several years between the onset of symptoms and a definitive diagnosis. In this respect, the revised scoring system of the American Society for Reproductive Medicine is normally employed to determine the disease stage (ranging from I, indicating minimal disease, to IV, indicating severe disease). This system is based on the type, location and appearance of the lesions, as well as the depth of the invasion caused and the extent of disease and adhesions (2,5,6). However, endometriosis symptoms do not always correspond to observations from laparoscopic exploration. The severity of these symptoms increase with age, along with the probability of a proper diagnosis. Moreover, the incidence of endometriosis peaks in women in their 40s (7). Which are the possible causes of the disease? Even though the underlying cause for endometriosis remains uncertain, it is likely to present a multifactorial origin. This includes inflammation enhanced by genetic causes, which may be epigenetically regulated, as well as triggered by exposure to environmental factors (3). So, it seems evident why pathophysiology of endometriosis keeps being a subject of debate. It remains unclear whether endometrial and endometriotic cells are genetically different, or whether such differences are the consequence of distinct environments or due to preexisting immunological defects (8). However, several hypotheses have been proposed to explain the origin of the disease:
This was the first hypothesis proposed, put forth as the main cause for the pathogenesis of endometriosis. Retrograde menstruation appears when viable endometrial fragments are driven through the Fallopian tubes, possibly by a pressure gradient originating from dys-synergic uterine contractions. Once these fragments reach the peritoneal cavity they can implant, grow and invade pelvic structures. The likelihood of this event is influenced epidemiologically by any menstrual, reproductive or personal factor that may augment pelvic contamination by regurgitated endometrium (Figure 1). Further support for this aetiology is derived from studies of obstructed or compromised outflow tracts (9,10,11). However, this event occurs in 76–90% of women with patent Fallopian tubes, and not all of them suffer from endometriosis (11).
The monthly regeneration of the endometrium after menstrual shedding and re-ephitelialization after parturition or surgical curettage supports the existence of a stem cell pool. The involvement of these cells in the formation of endometriotic deposits could be the result of abnormal translocation of the normal stratum basalis of the endometrium via retrograde menstruation. Some group of cells may deposit and survive in the peritoneal cavity after retrograde flow, and may reactivate during adolescence in response to ovarian hormones. However, there are currently no data on the amount of endometrial stem/progenitor cells in neonatal period compared to the adult endometrium (11).
This theory postulates that endometriosis originates from the metaplasia of specialised cells present in the mesothelial lining of the visceral and abdominal peritoneum. Hormonal or immunological factors are thought to stimulate the transformation of normal peritoneal tissue/cells into endometrium-like tissue. The theory may explain the occurrence of endometriosis in pre-pubertal girls. However, the usual driving force for endometrial growth, oestrogen, is not present in pre-pubertal girls, and therefore this condition may be different from the endometriosis found in women of reproductive age. Nevertheless, this theory is imperfect due to endometriotic lesions being found in areas outside the course of the Müllerian duct (4,11).
Genetic factors represent about half of the variation in endometriosis risk, with an estimate of heritability of 51%. Meta-analyses of the few genome-wide studies performed in the past few years have provided evidence of a robust association of endometriosis with seven risk loci. Among them, WNT4, CDKN2B-AS1 and GREB1 are of particular interest due to their gene-based ranking, known pathophysiology and proximity to SNPs of genome-wide significance. Therefore, these genes represent strong candidates for further studies on endometriosis (4,12,13). Inflammation is an additional typical feature of endometriosis, since the presence of ectopic tissue in the peritoneal cavity is associated with overproduction of prostaglandins, cytokines and chemokines. Macrophages infiltrating the ectopic lesions express typical markers of alternative activation, favouring the growth of the lesions and promoting associated angiogenesis. Overproduction of reactive oxygen species (ROS) is also accompanied by a decreased level of antioxidants that usually eliminates these molecules. Thus, the resulting accumulation of ROS may contribute to the propagation and maintenance of endometriosis and associated symptoms (4,10,11). Oestrogens fuel ectopic endometrium growth, and alterations in oestrogen signalling have been associated with the disease. In fact, it is known that oestradiol produced both in the steroidogenic organs and locally in the endometriotic implants through aromatase expression promote the growth of endometrial tissue ectopically (4,11). This ectopic tissue has been consistently shown to express different levels of oestrogen receptors (ER) α and β than eutopic tissue, being ERβ highly present in ectopic tissue (4). Deficient methylation of the promoter of the ERβ-encoding gene has been suggested to result in pathological overexpression of ERβ in endometriosis, which in turn suppresses ERα expression and diminishes oestradiol-mediated induction of the progesterone receptor in endometriotic cells. This mechanism is thought to contribute to resistance to selective actions of progesterone in these cells, which is manifested by perturbations in a number of downstream progesterone target genes (4,11). Progesterone normally triggers a uterine endometrial response characterized by inhibition of oestrogen-dependent proliferation of epithelial cells, secretory maturation of the glands, and transformation of stromal cells into specialized decidual cells. Moreover, progesterone transiently induces a receptive phenotype in endometrial epithelial cells essential for embryo implantation [you can read more about the role of these hormones in the endometrium in our previous publication here]. As a consequence of progesterone resistance, genes critical to these events, such as prolactin for decidual response or glycodelin for embryo implantation, are dysregulated in the endometrium of affected women. Endometriosis-derived inflammation, in turn, could induce progesterone resistance by altering the signalling pathway of this hormone through mechanisms of competition or interference with proinflammatory transcriptional factors (4,11,14,15,16). The observation that autoimmune diseases tend to be more common in women with endometriosis supports the hypothesis that pathogenesis of this condition may involve a defective immune response in these patients. Women suffering from endometriosis present higher concentration of activated macrophages, decreased cellular immunity and repressed NK cell function (11). Endometriosis and infertility The relationship between endometriosis and infertility has been debated for many years. Infertile women are 6-8 times more likely to suffer from endometriosis than fertile women (7). Despite extensive research no agreement has been reached, and several mechanisms have been proposed to explain the association between endometriosis and infertility. These mechanisms include distorted pelvic anatomy, endocrine and ovulatory abnormalities, altered peritoneal function and altered hormonal and cell-mediated functions in the endometrium. Major pelvic adhesions or peritubal adhesions disturbing the tube-ovarian liaison and tube patency can impair the release of oocytes from the ovary, inhibit oocyte pickup, or impede the transport of the ovum itself (7). Women with endometriosis may exhibit endocrine and ovulatory disorders, including luteinized unruptured follicle (LUF) syndrome, impaired folliculogenesis, luteal phase defect, and premature or multiple LH surges. Moreover, a complex network of humoral and cellular immunity factors modulates the growth and inflammatory behaviour of ectopic endometrial implants, and so it may have adverse effects on the function of the oocyte, sperm, embryo, or Fallopian tubes (7,16). Management of endometriosis by assisted reproductive technologies There is currently no clear answer to the question of whether endometriosis has a negative impact on IVF outcomes. Several studies have previously suggested poorer outcomes in comparison to control cases, whereas other have shown no significant differences (17). Clinical outcomes for different stages of endometriosis Patients with endometriosis can present different levels of severity, which have a strong influence in the outcomes. Thus, it would be common to find a case of disease at a more severe phase with worse results than a different one presenting less extensive endometriosis (18,19). In stage III/IV endometriosis the prognosis for IVF/ICSI treatments is lower compared to milder stages I/II. (19). In their retrospective study, Opøien et al. highlighted the fact that patients with a more severe form of the disease had fewer oocytes retrieved, despite the higher gonadotropin doses these women had been administered (20). This may be due to endometriosis affecting both oestrogen and progesterone mRNA receptors in granulosa cells (21). Likewise, patients suffering from stage III/IV endometriosis have been reported to show a decrease in implantation and clinical pregnancy rates (22). Endocrinology of endometriosis Measurements of circulating hormone concentrations have shown statistically higher levels of hMG/FSH in endometriosis patients than in control patients. However, both high-quality embryo and clinical pregnancy rates were found to be lower in such patients (23). Similarly, the high expression of PR-A and ER-α in patients with endometriosis might be a leading cause of ovarian dysfunction due to this condition. This means that stages III-IV patients required higher gonadotropin stimulation doses to prevent ovarian dysfunction (24). Endometriomas Endometriomas represent an additional variable that may also affect ART outcomes. They have been reported to affect 17-44% of patients with endometriosis, who exhibit reduced ovarian response due to the low response to gonadotropin stimulation (25). Such response has been widely discussed by different authors. Conclusions from these reports suggest a reduced number of retrieved oocytes in women with bilateral endometriomas, as well as the rates of top-quality embryos, implantation, clinical pregnancy and live birth, when compared to control groups (26,27,28). Gonadotropin stimulation for IVF in the endometriosis context Patients with stage III/IV endometriosis normally undergo stimulation by higher doses of gonadotropin, which consequently results in higher circulating oestradiol levels (24). D'Hooghe and coworkers performed an analysis of this kind of patients and demonstrated that the cumulative endometriosis recurrence rate (CERR) was lower after ovarian hyperstimulation for IVF than after lower-dose ovarian stimulation for IUI. This suggests that temporary exposure to high oestradiol levels during ovarian hyperstimulation for IVF is not a risk factor for endometriosis recurrence in women subjected to ART (29). Previous reports from Benaglia et al. have shown that after 3-6 months of IVF cycles 77% of patients experimented an improvement of the condition, whereas about 11% reported worsening. Also, it should be noted that endometrioma size also remained stable after IVF cycles, which suggests they are not affected by gonadotropin stimulation (30). IVF outcomes after medical therapy for endometriosis Medical interventions have been demonstrated to have benefit in alleviating, if not eliminating, symptoms associated with endometriosis (31). The first thing to control is the prolonged use of GnRHa prior to initiation of gonadotropin stimulation for ART. The extension of GnRHa use up to about 3 months has been reported to exhibit higher implantation rates and significantly higher clinical pregnancy rates (32). This is due to the fact that endometriosis patients were more likely to present aberrant endometrial expression of β3 integrin, and that a 3-month course of GnRHa allowed to rescue up to 64% of the expression (33). Another approach employed to increase integrin expression is the of danazol as a post-treatment after the ovulatory cycle. This has been reported to result in both similar clinical pregnancy and live birth rates to those from patients with normal integrin expression (34). A different medical therapy is the administration of oral contraceptives in women with endometriosis before the initiation of the actual ART treatment. This approach seems to improve clinical outcomes, keeping them comparable to women of similar age without endometriosis. In contrast, ART outcomes are markedly compromised in endometriosis patients who are not pretreated with this method. It is worth to mention that ovarian responsiveness to stimulation was not altered by 6-8 weeks use of oral contraceptives prior to initiation of ART treatment, including poor responders with endometriomas (35). So far, it has not been possible to establish the optimal duration of medical therapy for endometriosis by means of comparative trials. As a consequence, ideal patients who could benefit from medical intervention have not yet been depicted. In spite of this, it would be reasonable to think that those patients suffering from more severe stages of the disease and/or with prior implantation failure might be the best candidates (36). Infertility in women affected by endometriosis may be related to alterations in follicles, poor oocyte quality (...), or even decreased endometrial receptivity. Impact of surgical management of endometriosis on IVF outcomes Previous reports have shown that pre-cycle surgical intervention may result beneficial for the final outcome. Opøien et al. demonstrated that patients with stage I/II endometriosis treated with surgical resection presented higher clinical pregnancy rates than those who had only been subjected to diagnostic laparoscopy before IVF/ICSI (37). Similar data were obtained when evaluating results from a group of 825 endometriosis patients; those treated with surgical resection presented overall significantly higher pregnancy and IVF rates when compared to those who had been subjected to IVF alone, and also to those with no treatment whatsoever (38). Implantation and pregnancy rates have also been reported to increase after resection in patients with deeply invasive endometriosis, although this group needed higher gonadotropin doses for stimulation, and yet fewer oocytes were retrieved (39). However, it is important to keep in mind that research is limited by a variety of factors, such as variations in surgical techniques (i.e., ablation vs. resection), degree of removal of the endometriotic tissue or differences in IVF laboratories (40). Interestingly, previous reports indicate that IVF implantation rates are not affected by the time intervals between surgical interventions for resection of endometriosis in the absence of endometriomas (41). On the other hand, certain studies have reported the negative impact of surgical management of endometriomas on IVF treatments, like the inability to access follicles at oocyte retrieval following precycle resection of endometriomas, or the harmful effect on oocytes after exposure to endometrioma fluid. Nevertheless, most authors refuse these arguments (42), and few studies assert the benefits of surgery in endometriomas larger than 3 cm in order to treat painful symptoms or to facilitate access to the ovary (43). Current data from clinical outcomes suggest that, under controlled circumstances, IVF cycles are not compromised by the presence of endometriosis. The exception to this finding is the fact that patients with ovarian endometriomas showed lower response to gonadotropin stimulation (17). Thorough meta-analyses through early studies revealed lower number of oocytes obtained after egg collection, as well as decreasing fertilization, implantation and pregnancy rates in patients affected by endometriosis after ART treatments (18). However, it is important to note that pregnancy rates were extremely low in those years. Effects of endometriosis on ART outcomes Since endometriosis patients have sometimes been studied simultaneously to other groups of patients such as women suffering from Fallopian tube-related infertility, it is not clear whether endometriosis actually affects implantation rates. Barcelo and coauthors’ explanation is the similar percentage of meiotic abnormalities in in vitro matured oocytes between endometriosis patients and the control group after ovarian stimulation (44). An additional factor that might contribute to confusion is the presence of adenomyosis, which is frequently found in endometriosis patients and could have a deleterious impact on the implantation process (45). Altered ovulation and oocyte production, as well as increased inflammatory cells in the peritoneal fluid of endometriomas have been observed in endometriosis patients (46). In fact, infertility in women affected by endometriosis may be related to alterations on follicles, poor oocyte quality and related failures during subsequent embryogenesis, or even decreased endometrial receptivity. Such hypothesis is supported by the altered progesterone and cytokine concentrations found in the follicular fluid from these patients (44). Embryos derived from affected women are likely to develop more slowly, compared to embryos derived from women suffering from tubal disease (45). It is worth to mention that women with moderate to severe endometriosis who receive oocytes from healthy donors seem to present normal endometrial receptivity and pregnancy rates. Conversely, when donor oocytes from endometriosis-affected women are transferred into healthy women, implantation rates are lower and embryo quality is reduced (46). Further studies are needed, though, in order to determine pregnancy rates from donors in different conditions and disease stages (16). Delayed histological maturation or biochemical disturbances may lead to endometrial dysfunction, too. This is concluded from reports that show uterine implantation being affected by changes in receptivity on an endometriosis background (17). Endometrial expression of the adhesion molecule αvβ integrin has been observed to be reduced during the time of implantation in some endometriosis-affected women. Additionally, the synthesis of the endometrial ligand for L-selectin has also been observed to be affected in some patients (16). L-selectin is a trophoblast surface-coating protein, which may explain the altered implantation rates observed in such cases (47). The observation of luteal phase disruption associated to endometriosis may be due to dysregulation of the progesterone receptor, as well as an effect on progesterone target genes that consequently results in a decrease in endometrial receptivity (17,47). Sperm quality and/or function is also reduced, which has been proposed to be due to inflammatory/toxic effects of the peritoneal fluid, along with a higher amount of activated macrophages. Not only are these effects harmful to oocytes and sperm, but toxic to the embryo (17). Treatment of endometriosis-associated infertility IVF is currently the most effective treatment for endometriosis-associated infertility (17). However, comparison of data on the effectiveness of IVF for endometriosis patients vs. patients suffering from other causes of infertility is not without controversy. Reports from the Society of Assisted Reproductive Technology (SART) have shown that the average delivery rate per retrieval for patients undergoing IVF-ET is 39.1% for endometriosis-affected women, as opposed to 33.2% for women with other causes of infertility (48). Pre-treatment ovulation suppression is a possibility to be considered in order to enhance suppression of inflammatory cytokines, as well as to reduce the presence of disease signs prior to any form of ART. Nevertheless, further research will be required on patients with endometriomas to assess their effect on IVF/ICSI, and to elucidate whether pre-ART surgical intervention may increase success rates (48). Potential treatments in the future There is currently no consensus on whether performing surgery prior to undergoing ART is fundamental for achieving pregnancy. Either way, there is a priority in terms of age in endometriosis cases (17). There are, however, some novel medical therapies, such as immunoconjugate (ICON) and aromatase inhibitors. ICON targets aberrantly expressed tissue factor on endometriotic endothelium, causing regression of the established disease (most likely by devascularization), which seems to improve fertility rates (17,49). Aromatase inhibitors, absent under normal circumstances, are found to be present in ectopic endometrial tissue; this may have a direct impact on oestradiol levels and implantation rates in endometriosis patients (50,51). Current treatment of endometriosis-associated infertility focuses on improving fecundity by removing or reducing ectopic endometrial implants, thus restoring normal pelvic anatomy (47). There are several possibilities that practitioners can adopt when facing this kind of events, depending on the particular case and the patient: expectant management, medical treatment and/or surgical treatment (48,52). The reality is that the optimal method of choice to treat endometriosis-associated infertility is an individualized decision that should be made on the basis of the specificity of the patient (18,50). CONCLUSIONS Despite lower ovarian response, reduced embryo quality and impaired implantation in moderate/severe cases, endometriosis patients have been able to obtain IVF/ICSI success rates similar to those with tubal factor-related infertility. As it has been widely explained, the combination of aggressive but controlled ovarian hyperstimulation, appropriate hypophysis suppression and efficient surgery before initiating cycles seemed to be crucial and significantly efficient for IVF/ICSI success on patients suffering from endometriosis (50,52). Within the last few years, scientific knowledge have made it possible to develop certain clinical improvements that have surely opened new possibilities for endometriosis patients. REFERENCES 1. Available from: https://www.womensmd.org/wp-content/uploads/2017/06/Endometriosis-causing-heavy-periods-with-blood-clots.jpg [Cited November 4 2017].
2. Kennedy S, Bergqvist A, Chapron C, d’Hooghe T, Dunselman G, Greb R, et al. ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod. 2005;20:2698–704. 3. Johnson NP, Hummelshoj L, World Endometriosis Society Montpellier Consortium. Consensus on current management of endometriosis. Hum Reprod. 2013;28:1552–68. 4. Vercellini P, Viganò P, Somigliana E, Fedele L. Endometriosis: pathogenesis and treatment. Nat Rev Endocrinol. 2014;10(5):261–75. 5. Giudice L. Endometriosis. N Engl J Med. 2010;362:2389–98. 6. Practice Committee of the American Society for Reproductive Medicine. Endometriosis and Infertility. Fertil Steril. 2006;14:S156–60. 7. Bulletti C, Coccia ME, Battistoni S, Borini A. Endometriosis and infertility. J Assist Reprod Genet. 2010; 27:441–7. 8. Koninckx P, Ussia A, Adamyan L, Wattiez A, Donnez J. Deep endometriosis: definition, diagnosis, and treatment. Fertil Steril. 2012;98(3):564-571. 9. Burney R, Giudice L. Pathogenesis and pathophysiology of endometriosis. Fertil Steril. 2012;98(3):511-519. 10. Lebovic D, Mueller M, Taylor R. Immunobiology of endometriosis. Fertil Steril. 2001;75(1):1-10. 11. Sourial S, Tempest N, Hapangama D. Theories on the Pathogenesis of Endometriosis. Int J Reprod Med. 2014; 179515.1-9. 12. Nyholt DR, Low SK, Anderson CA, Painter JN, Uno S, Morris AP et al. Genome-wide association meta-analysis identifies new endometriosis risk loci. Nat Genet. 2012;44(12):1355–1359. 13. Pagliardini L, Gentilini D, Vigano’ P, Panina-Bordignon P, Busacca M, Candiani M et al. An Italian association study and meta-analysis with previous GWAS confirm WNT4, CDKN2BAS and FN1 as the first identified susceptibility loci for endometriosis. J Med Genet. 2013;50:43–46. 14. Aghajanova L, Hamilton A, Kwintkiewicz J, Vo KC, Giudice LC. Steroidogenic enzyme and key decidualization marker dysregulation in endometrial stromal cells from women with versus without endometriosis. Biol Reprod. 2009;80:105 –114. 15. Wei Q, St Clair JB, Fu T, Stratton P, Nieman LK. Reduced expression of biomarkers associated with the implantation window in women with endometriosis. Fertil Steril. 2009;91: 1686–91. 16. Practice Committee of the American Society for Reproductive Medicine. Endometriosis and infertility: a committee opinion. Fertil Steril. 2012; 98: 591-598. 17. Surrey ES. Endometriosis and assisted reproductive technologies: maximizing outcomes. Semin Reprod Med. 2013;31:154–63. 18. Barnhart K, Dunsmoor-Su R, Coutifaris C. Effect of endometriosis on in vitro fertilization. Fertil Steril. 2002;77:1148 –1155. 19. Kuivasaari P, Hippelainen M, Anttila M, Heinonen S. Effect of endometriosis on IVF/ICSI outcome: stage III/IV endometriosis worsens cumulative pregnancy and live-born rates. Hum Reprod. 2005;20:3130–3135. 20. Opøien HK, Fedorcsak P, Omland AK, Abyholm T, Bjercke S, Ertzeid G, et al. In vitro fertilization is a successful treatment in endometriosis-associated infertility. Fertil Steril. 2012;97:912–8. 21. Karita M, Yamashita Y, Hayashi A, Yoshida Y, Hayashi M, Yamamoto H et al. Does advanced-stage endometriosis affect the gene expression of estrogen and progesterone receptors in granulosa cells? Fertil Steril. 2011;95:889 – 894. 22. Harb H, Gallos I, Chu J, Harb M, Coomarasamy A. The effect of endometriosis on in vitro fertilisation outcome: a systematic review and meta-analysis. BJOG. 2013;120:1308–20. 23. Revelli A, Pettinau G, Basso G, Carosso A, Ferrero A, Dallan C et al. Controlled Ovarian Stimulation with recombinant-FSH plus recombinant-LH vs. human Menopausal Gonadotropin based on the number of retrieved oocytes: results from a routine clinical practice in a real-life population. Reprod Biol Endocrinol. 2015;13:77. 24. Tan CW, Lee IH, Choolani M, Tan HH, Griffith L, Chan J. Endometriosis, endometrium, implantation and fallopian tube. Hum Reprod. 2013;28:206-226. 25. Somigliana E, Infantino M, Benedetti F, Arnoldi M, Calanna G, Ragni G. The presence of ovarian endometriomas is associated with a reduced responsiveness to gonadotropins. Fertil Steril. 2006;86:192–196. 26. Benaglia L, Bermejo A, Somiglianaetal E. Invitrofertilization outcome in women with unoperated bilateral endometriomas. Fertil Steril. 2013;99:1714–1719. 27. Suzuki T, Izumi SI, Matsubayashi H, Awaji H, Yoshikata K, Makino T. Impact of ovarian endometrioma on oocytes and pregnancy outcome in in vitro fertilization. Fertil Steril. 2005;83:908–913. 28. Almog B, Shehata F, Sheizaf B, Tan SL, Tulandi T. Effects of ovarian endometrioma on the number of oocytes retrieved for in vitro fertilization. Fertil Steril. 2011;95:525–527. 29. Hooghe MD, Denys B, Spiessens C, Meuleman C, Debrock S. Is the endometriosis recurrence rate increased after ovarian hyperstimulation? Fertil Steril. 2006;86:283–290. 30. Benaglia L, Somigliana E, Santi G, Scarduelli C, Ragni G, Fedele L. IVF and endometriosis-related symptom progression: insights from a prospective study. Hum Reprod. 2011;26:2368–2372. 31. Mehedintu C, Plotogea M, Ionescu S, Antonovici M. Endometriosis still a challenge. J Med Life. 2014;7:349-57. 32. Surrey ES, Silverberg KM, Surrey MW, Schoolcraft WB. Effect of prolonged gonadotropin-releasing hormone agonist therapy on the outcome of in vitro fertilization-embryo transfer in patients with endometriosis. Fertil Steril. 2002;78:699–704. 33. Lessey BA. Medical management of endometriosis and infertility. Fertil Steril. 2000;73:1089–1096. 34. Tei C, Maruyama T, Kuji N, Miyazaki T, Mikami M, Yoshimura Y. Reduced expression of alphavbeta3 integrin in the endometrium of unexplained infertility patients with recurrent IVF-ET failures: improvement by danazol treatment. J Assist Reprod Genet. 2003;20:13-20. 35. Ziegler D, Gayet V, Aubriotetal FX. Useoforalcontraceptives in women with endometriosis before assisted reproduction treatment improves outcomes. Fertil Steril. 2010;94:2796–2799. 36. Furness S, Yap C, Farquhar C, Cheong Y. Pre and post-operative medical therapy for endometriosis surgery. Cochrane Database Syst Rev. 2004:CD003678. 37. Opøien HK, Fedorcsak P, Byholm T, Tanbo T. Complete surgical removal of minimal and mild endometriosis improves outcome of subsequent IVF/ICSI treatment. Reprod Biomed Online. 2011;23:389 – 395 38. Barri PN, Coroleu B, Tur R, Barri-Soldevila PN, Rodríguez I. Endometriosis-associated infertility: surgery and IVF, a comprehensive therapeutic approach. Reprod Biomed Online. 2010;21:179–185. 39. Bianchi PH, Pereira RM, Zanatta A, Alegretti JR, Motta EL, Serafini PC. Extensive excision of deep infiltrative endometriosis before in vitro fertilization significantly improves pregnancy rates. J Minim Invasive Gynecol. 2009;16:174–180. 40. Surrey ES, Schoolcraft WB. Does surgical management of endometriosis within 6 months of an in vitro fertilization–embryo transfer cycle improve outcome? J Assist Reprod Genet. 2003;20:365–70. 41. Khamsi F, Yavas Y, Lacanna IC, Roberge S, Endman M, Wong JC. Exposure of human oocytes to endometrioma fluid does not alter fertilization or early embryo development. J Assist Reprod Genet. 2001;18:106-109. 42. Benschop L, Farquhar C, Van der Poel N, Heineman MJ. Interventions for women with endometrioma prior to assisted reproductive technology. Cochrane Database Syst Rev. 2010;11:CD008571. 43. Elter K, Oral E. Surgical treatment before assisted reproductive technologies. Semin Reprod Med. 2014; 32(04): 253-261. 44. Barcelos ID, Vieira RC, Ferreira EM, Martins WP, Ferriani RA, Navarro PA. Comparative analysis of the spindle and chromosome configurations of in vitro-matured oocytes from patients with endometriosis and from control subjects: a pilot study. Fertil Steril. 2009:92;1749–1752. 45. Salim R, Riris S, Saab W, Abramov B, Khadum I, Serhal P. Adenomyosis reduces pregnancy rates in infertile women undergoing IVF. Reprod BioMed Online. 2012;25:273– 277. 46. Dmowski WP, Pry M, Ding J, Rana N. Cycle specific and cumulative fecundity in patients with endometriosis who are undergoing controlled ovarian hyperstimulation-intrauterine insemination or in vitro fertilization-embryo transfer. Fertil Steril. 2002;78:750-756. 47. Macer ML, Taylor HS. Endometriosis and infertility: a review of the pathogenesis and treatment of endometriosis-associated infertility. Obstet Gynecol Clin North Am. 2012;39: 535-549. 48. Ruiz Flores FJ, Garcia-Velasco JA. Is there a benefit for surgery in endometrioma associated infertility?. Curr Opin Obstet Gynecol. 2012;24(3):13640. 49. Hadman M, Omar SZ, Dunselman G, Chenog Y. Influence of endometriosis on assisted reproductive technology outcomes: a systematic review and meta-analysis. Obstet Gynecol. 2015;125(1):79-88. 50. Wahd SA, Alaf SK, Al-Shawaf T, AlTawil NG. Ovarian reserve markers and assisted reproductive technique (ART) outcomes in women with advanced endometriosis. Reprod Biol Endocrinol. 2014;12:120. 51. Kawwass JF, Crawford S, Session DR, Kissin DM, Jamieson DJ. Endometriosis and Assisted Reproductive Technology: United States Trends and Outcomes: 2000–2011. National ART Surveillance System Group. Fertil Steril. 2015;103(6):1537-43. 52. D Xiyuan, L Xiuhua, Wang R, Zhang H. The impact of endometriosis on IVF/ICSI outcomes. Int J Clin Exp Pathol. 2013;6(9):1911-1918.
4 Comments
|
Entries
March 2019
Categories
All
 2016-2019. All Rights Reserved by Embryologist Media. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License . |
Embryologist Media

{kind=link}