|
Authors: Iris Martínez Rodero and Raquel Pillado González "Selection of the best spermatozoon for ICSI is critical and it is directly linked to fertilization rates, optimal embryo development and implantation rates" 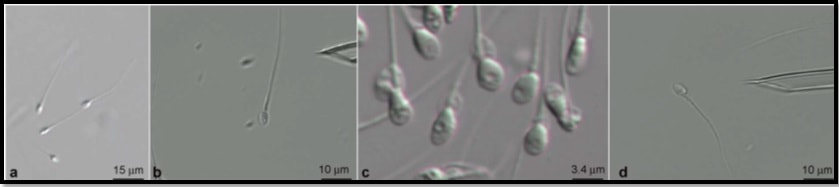 Figure 1. Spermatozoa observed at low magnification (a) and high magnification (b–d). The shape and presence of vacuoles can be clearly observed in (c). A vacuole-free spermatozoon is shown in (d). INTRODUCTION It is estimated that approximately 10% of couples seek help to overcome infertility problems. Data from the American Society of Reproductive Medicine points to male factor as the reason behind one third of couples’ infertility problems (1). The remaining two thirds seem to be equally distributed between female-related problems and a mixture of unexplained causes and combinations of male and female factors, respectively (1). As continuation of our previous post on sperm selection, we revisit the topic from the perspective of the numerous techniques currently available to be specifically used prior intracytoplasmic sperm injection (ICSI). This procedure is the advised treatment for most cases of male factor infertility; in fact, ICSI accounts for 70-80% of cycles performed globally (2). ICSI candidates often present low sperm count and/or increased probability of genetic abnormalities, compromised DNA and morphological defects of spermatozoa. Therefore, selection of the best spermatozoon for ICSI is critical and it is directly linked to fertilization rates, optimal embryo development and implantation rates (3). Traditional sperm selection procedures (swim-up and density gradient centrifugation (DGC)) are based just on motility rather than molecular features. Consequently, in order to choose the best spermatozoa, researchers have developed different non-invasive methods to process and select sperm for ICSI (Table 1) (2). 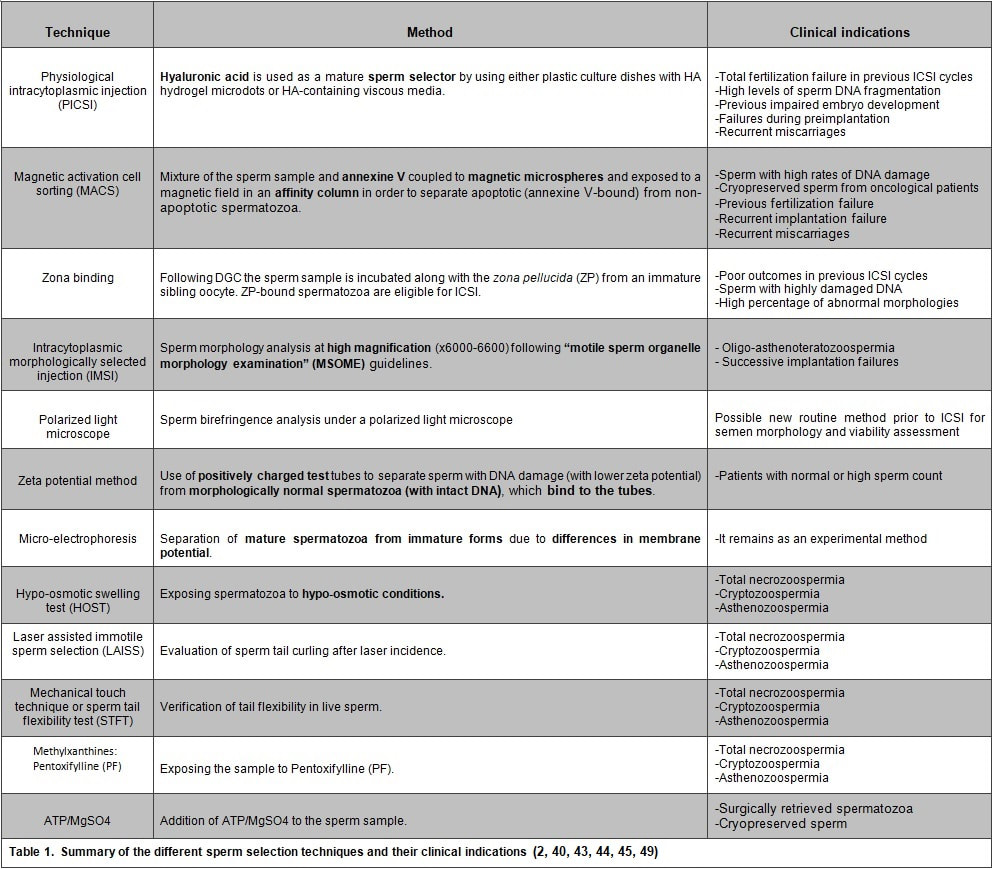 SPERM SELECTION TECHNIQUES Sperm selection prior to fertilization is a crucial step for IVF success, especially in cases of low number of available oocytes to inject (4). Several techniques are currently utilised for this purpose, each of them relying on different features in order to select the optimal sperm. BINDING ASSAY TECHNIQUES Physiological intracytoplasmic injection (PICSI) This technique is based on the fact that hyaluronic acid (HA) plays an important role in selecting functionally competent sperm during in vivo fertilization (5). Not only HA is the main component of the cumulus matrix that surrounds the human oocyte, but also a natural selector of developmentally mature sperm. Furthermore, experimental data have shown that it can be used with a similar effect in vitro. HA-binding spermatozoa in vitro exhibit complete plasma membrane remodelling, decreased levels of cytoplasmic inclusions and residual histones, nuclear maturation and reduced risk of chromosome imbalance (i.e. chromosomal aneuploidy) and chromatin diseases (4). Currently, there are two options available to perform this technique. First, plastic culture dishes with HA hydrogel microdots attached to the bottom. After using this method the desired spermatozoa remain bound to the microdots by the head, while flagella beat in place (4). Secondly, the use of an alternate HA-containing viscous medium, method known as “Sperm Slow” because the spermatozoa appear “slowed down” (4). Since PICSI is considered to better assess the physiological potential in order to select sperm for ICSI, some authors claim it should replace the use of conventional ICSI and potentially toxic polyvinylpyrrolidone (PVP) (used to slow down sperm movement). Nevertheless, significant improvement of IVF outcomes using HA-based sperm selection is still to be confirmed in larger studies (6, 7), reason why the use of PICSI is currently limited to punctual cases in which significant improvement of clinical outcomes has been proved (8). Such cases include total fertilization failure by ICSI, high levels of DNA fragmentation, impaired embryo development, failure to implant in the uterus and recurrent miscarriages (9, 10). Fertilization failure after ICSI can sometimes be explained by problems in sperm nucleus decondensation and chromatin abnormalities related to DNA fragmentation (11). Sperm with such DNA damage and/or chromosome unbalance are avoided by PICSI/HA binding negative selection (3). Although it is a controversial issue, several authors have found a significant improvement of embryo quality and implantation ability when performing PICSI vs conventional ICSI, as well as a reduced number of miscarriages (3, 11, 12, 13, 14). The decreased incidence of miscarriages seems to be linked to the incapacity of sperm with genetic defects to form a normal pro-nucleus after conventional ICSI, thus generating aneuploid embryos with high levels of fragmentation during cleavage. Such aberrant embryos normally end up in pregnancy loss (14). Since PICSI allows for selection of sperm with properly compacted chromatin, embryos derived from these spermatozoa are less likely to present defects in quality (15). This translates into a higher implantation potential and a lower incidence of miscarriage, which eventually improves the reproductive outcome (12, 13). Magnetic activation cell sorting (MACS) In 2008 Said and colleagues proposed a protocol combining a new method, denominated magnetic activation cell sorting (MACS), and density gradient column (DGC) in order to obtain higher-quality sperm samples (2). MACS consists in mixing up the semen sample with annexine V (A5) (known to have high affinity with phosphatidylserine (PS)) coupled to magnetic microspheres. The sample is then exposed to a magnetic field in an affinity column (16). A5-bound sperm have been linked to PS externalisation, a well-known sign of apoptosis due to the loss of membrane integrity. MACS should be performed prior to DGC because PS externalisation naturally occurs during sperm capacitation by DGC, and so MACS may inadvertently discard good-quality sperm (17). During the last decade, several studies have corroborated the efficient use of this protocol in order to obtain sperm samples with a low DNA fragmentation index and higher fertilization potential (2, 16). Because MACS reduces the percentage of apoptotic sperm selected from the sample, this technique is mostly indicated in cases of high rates of DNA damage or predisposition to suffer from it (18). Such cases include: patients with altered sperm parameters, cryopreserved spermatozoa from cancer patients (19), previous fertilization failure, recurrent implantation failure and recurrent miscarriage (20, 21). Several clinics have implemented MACS in their daily routine, claiming selection of sperm through MACS to improve their ICSI outcome (22, 23, 24). However, such statement remains controversial, since other authors have reported no actual beneficial effect after using this technique (16, 25). Zona binding This method mimics natural sperm selection using the zona pellucida (ZP) from an immature sibling oocyte (26). The sperm sample is processed by DGC and then incubated along with the ZP for two hours. ZP-bound sperm are then eligible for ICSI. Although various studies have linked the ZP binding assay prior to ICSI to improved embryo quality and implantation rate, it is still not feasible to employ this method on a routine basis due to the extra amount of work and time required. Therefore, it is currently recommended to remain restricted to patients with poor outcomes in previous ICSI cycles, or to those who exhibit sperm with damaged DNA or abnormal morphologies (2). MICROSCOPY BASED TECHNIQUES Intracytoplasmic morphologically selected injection (IMSI) Studies have shown that sperm classified as morphologically “normal” at conventional optical resolution and magnification (x200-x400) may carry ultrastructural defects. Many of these abnormalities have been linked to hidden chromosomal defects, high levels of DNA fragmentation, abnormal centriolar function, etc. (1, 2). These aberrations may impede fertilization, lead to post-fertilization arrest or even disrupt embryo development (2). IMSI is an approach developed from a method of sperm evaluation, first described in 2002 by Bartoov and colleagues and denominated “motile sperm organelle morphology examination” (MSOME) (27). In order to apply this evaluation technique, observations need to be performed at x6000-6600 magnification (1). Performance of sperm selection along with MSOME requires the use of specific equipment. This should be an inverted light microscope with high-power optics intended for differential interference contrast and enhanced by digital imaging, which allows the embryologist to assess sperm morphology in real time. Sperm selection is carried out in a dish different from the one used for ICSI; it is a glass-bottomed dish that allows for the best optimal quality. Semen samples for IMSI are subjected to discontinuous DGC beforehand, but the exact procedure may vary depending on the quality of the sample (2). Sperm selection based on IMSI—MSOME findings helps to discard spermatozoa with mitochondrial dysfunction or DNA damage (4). In this regard, IMSI-MSOME has been proved useful for oligo-asthenoteratozoospermic patients (28) and for couples with recurrent implantation failures, reducing miscarriage rates by 50% (29). Nevertheless, simpler techniques are available for selecting sperm with low DNA fragmentation such as PICSI and MACS, so IMSI-MSOME is not yet extendedly used (4). In fact, this technique did not have the expected impact due to its downsides: high cost and long time for selecting sperm for ICSI. Depending on semen quality, selection may take around 60-120 minutes, which could negatively affect cells given that sperm nuclei may vacuolize after 2-hour exposure to warm media (30). Polarized light microscope The different anisotropic properties of spermatozoa through its protoplasmic texture provoke polarized light to be refracted at different speeds. These differences between refractions are known as retardance or birefringence (31). Viable human spermatozoa are naturally birefringent, while this characteristic is absent in pathological, dead or necrotic ones due to changes in the molecular structures of the cell and/or organelles (nucleoprotein filaments, axoneme, mitochondria, etc.) (32, 33). Examined under polarized microscope (PM), a normal spermatozoon will exhibit a non-luminous acrosome and luminous and normal-sized compact nucleus and flagellum (Giulia Collodel 2010). Multiple studies support the correlation between sperm head birefringence and DNA fragmentation, fertilization rates and higher embryo quality (2). The increase of a sperm head retardance is positively correlated with DNA damage, the optimal value for sperm head retardance oscillates between 0.56 nm and 0.91 nm. (32). Thanks to improvements in polarized light microscopy it is now possible to evaluate viability, motility, morphology and concentration of a sperm sample, all in a single step and with no need of exposure to potentially harmful dyes or environmental conditions (33). MEMBRANE POTENTIAL BASED TECHNIQUES Zeta potential method Zeta potential refers to the negative electric potential observed between the outer medium and the sperm membrane surface. The sperm selection technique based on this potential was developed following the observation that sperm with damaged DNA exhibited a lower Zeta potential (34). This method consists in the use of positively charged test tubes to which morphologically normal spermatozoa containing intact DNA can bind (2). This promising, easy and time-efficient new method presents the major drawback of a low recovery rate (8.8%), which is especially troubling in cases of oligozoospermic patients, who represent a high percentage of ICSI candidates (34). Micro-electrophoresis During sperm maturation in the epididymis, capacitation and acrosome reaction, the sperm membrane undergoes specific modifications (35, 36), among which the addition of sialic acid residues is noteworthy. High concentrations of this residue reflect normal spermatogenesis and sperm maturation (37), as well as higher negative charge compared to immature or abnormal sperm (38). Taking advantage of such trait, negatively-charged spermatozoa are selected as they migrate towards the anode during electrophoretic sperm separation (39). Similarly to the Zeta-potential method, micro-electrophoresis enables the isolation of sperm with no DNA damage, since they present higher negative net charge (40). Although micro-electrophoresis remains an experimental method, the percentage of negatively charged sperm is directly associated with fertilization rate and blastocyst development and inversely associated with embryo arrest (41). ABSOLUTE IMMOTILE SPERM SELECTION TECHNIQUES: There are some cases of severe male factor infertility, such as total necrozoospermia, in which absolute immotile sperm are prevalent. In such cases, testicular sperm extraction (TESE) seems to be the only actual solution; however, obtaining motile and/or viable sperm for ICSI may result an impossible goal (42). Difficulties to select viable sperm can also occur in cases of severe cryptozoospermia and asthenozoospermia. Therefore, several techniques have been developed in order to differentiate immotile and non-viable sperm (2, 43, 44, 45). Hypo-osmotic swelling test (HOST) Studies have shown that in cases of severe male infertility normal sperm morphology will still likely have a high DNA fragmentation index. HOST is a method to estimate chromatin integrity (2), based on the degree of swelling of the cytoplasm and curling of the tail in live sperm when exposed to hypo-osmotic conditions. Different swelling patterns correspond to different degrees of chromatin integrity; by identifying these patterns, live spermatozoa with normal membrane function and low DNA fragmentation can be selected (2, 43). Laser assisted immotile sperm selection (LAISS) LAISS helps to differentiate between viable and dead spermatozoa by evaluating curling of the flagellum, as detected in live sperm when hit by the laser. The use of LAISS has reported results comparable to HOST; however, the former is much quicker than the latter, and its effect can be immediately observed without the need of continued evaluation, contrary to what is required for HOST (43). Mechanical touch technique or the sperm tail flexibility test (STFT) Although HOST is the most used test to differentiate live immotile spermatozoa from dead ones, evidence suggests that it may not be totally reliable (46, 47). Furthermore, solutions used for hypo-osmotic shock can be harmful for spermatozoa. In 2003, Soares and coauthors published their results using a simple and low-cost technique for selecting viable immotile sperm. They observed acceptable fertilization rates after injecting spermatozoa with flexible tail from total immotile sperm samples. Based on these results, the authors proposed STFT as a means to discriminate live from dead sperm; STFT consists in touching the flagellum with the ICSI pipette to check flexibility. Spermatozoa with flexible (non-stiff) flagellum may be considered alive and therefore eligible for ICSI (44). Methylxanthines: Pentoxifylline (PTX) Use of Pentoxifylline (PTX) enhances sperm motility by inhibiting the breakdown of cAMP which is essential for sperm motility (48). PTX is a 3’5’-nucleotide phosphodiesterase inhibitor that might result highly toxic for the oocyte or the embryo (2). Nevertheless, due to the reported increased fertilisation rates for immotile sperm after exposure to PTX (48), this method is still recommended for thawed testicular sperm samples, though only in cases of 100% immotile sperm, and always for short periods of time (2, 48). ATP/MgSO4 In 2014 Neri and colleagues proposed the use of ATP/MgSO4 solution for immotile spermatozoa that did not respond to motility enhancers (49). It is especially recommended for surgically retrieved or thawed sperm samples (49). The exposure to ATP/MgSO4 stimulate sperm kinetic machinery provoking viable, but immotile spermatozoa flagella to twitch (2). The same team reported that 64.6% of spermatozoa from an only immotile sperm sample exhibited flagellar movement after exposure to ATP/MgSO4 (49). CONCLUSIONS ICSI is a highly efficient technique, which reaches up to 85-90% fertilisation rates. Two main causes can explain fertilisation failure by this technique: the lack of appropriate sperm for injection or failed oocyte activation. Having covered the latter in a previous publication, the present post aims to review the current available techniques for the improved sperm selection for ICSI. Among these, IMSI, PICSI and MACS are widely studied, and their efficiency extensively accepted. Several novel approaches have been also developed. HOST, polarised microscopy and micro-electrophoresis are suggested to improve fertilisation rates, although multicenter randomised control trials will be needed before their general implementation to IVF routine. On the other hand, ZP binding assay and Zeta potential method are still experimental techniques that are yet to demonstrate their clinical advantages and feasibility. Finally, the best method for selecting live spermatozoa from totally immotile sperm samples remains a controversial issue. Whereas HOST seems to be the most extended one, simpler and easier techniques have appeared in the last decade that may also prove highly useful for an effective good-quality sperm selection. REFERENCES
3 Comments
|
Entries
March 2019
Categories
All
 2016-2019. All Rights Reserved by Embryologist Media. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License . |
Embryologist Media
